
|
|
1.IntroductionThe ability to confidently assess fetal oxygenation is of great importance to obstetricians, midwives, and parents. A deficiency of oxygen in fetal blood can lead to permanent brain damage, neurological disorders, or even death.1, 2 Although there are a number of methods currently used to determine fetal health, most are indirect monitors of fetal oxygenation. During times of uncertainty, physicians are forced to decide whether a fetus is in distress and if cesarean delivery is necessary based on the information available to them. Electronic fetal monitors (EFM) are commonly used for fetal heart rate monitoring, the standard for assessing fetal well-being. However, studies have shown that “nonreassuring” fetal heart rate patterns are not always indicative of fetal compromise. In fact, they have been associated with a high rate of false-positive ante partum assessment tests.1, 2, 3, 4 Fetal scalp blood sampling (FBS), which offers a measure of fetal pH (an indicator of fetal hypoxia), is invasive and can only provide intermittent information.2 Transvaginal fetal pulse oximetry is a newer method, which measures fetal arterial saturation by placing an optical sensor on the fetal head or cheek. However, this method can only be used during labor and can be unreliable due to motion and low perfusion.5 Transabdominal NIRS offers a noninvasive method to continuously monitor blood oxygen saturation and blood volume, in utero. Biological tissue is relatively transparent in the NIR region , allowing NIR photons to probe deeply before being absorbed or returning to the tissue surface.6, 7 Photons that do not return to the surface are absorbed by various tissue chromophores (e.g., water, hemoglobin, lipids, etc.). In the fetal brain, absorption is primarily due to oxy- and deoxy-hemoglobin (HbO and Hb, respectively).8 The use of multiple wavelengths and the knowledge of chromophore specific wavelength-dependent molar extinction coefficients allows for the determination of these chromophore concentrations.9 Several developments have been made to improve the ability of NIRS to offer more accurate quantitative information. Continuous-wave (cw) instruments require a priori knowledge of the baseline optical properties, or differential pathlength factor (DPF), in order to map amplitude measurements to absolute chromophore concentrations. The DPF is the absolute pathlength (dependent on the tissue optical properties, tissue geometry, and boundary conditions) divided by the optode spacing on the surface. Several investigators have measured this parameter for various tissue types. However, variability in baseline blood volume and saturation among individuals yields uncertain results.10, 11, 12 Frequency-domain (FD) methods13 and time-resolved spectroscopy (TRS)14, 15 acquire absorption and scattering properties by fitting phase and temporal measurements, respectively, to theoretical models based on the diffusion equation.16 The quantitative accuracy of the FD and TRS methods, therefore, relies on the theoretical model used to estimate the baseline optical properties. Accurately quantifying cerebral blood saturation in adults, neonates,17 or the fetus (transabdominally) is challenging, regardless of the NIR instrumentation used. Previous studies have demonstrated, through simulations,18, 19, 20, 21, 22 phantom models,23 and in vivo experiments,22, 24 the feasibility of detecting NIR photons that have penetrated an underlying fetal layer, centimeters deep. There has been a discussion among investigators as to which photon diffusion model most accurately describes photon propagation through a two-layer model,11, 12, 14, 16, 22 such as that described here. In a study by Choe 25 a multiseparation, frequency-domain NIR instrument was employed to obtain cerebral blood saturation measurements of an ovine fetus at various stages of hypoxia, in utero. A numerical solution was used to solve the diffusion equation for the two-layer model. Several assumptions were made about the baseline optical properties of both the maternal and fetal layers, in order to quantify NIR blood saturation measurements. The goal of this study is to demonstrate the feasibility of quantifying NIR transabdominal fetal blood saturation measurements, assuming there is uncertainty in the chosen baseline optical properties, and to investigate the error propagation due to incorrect baseline assumptions. A pregnant ewe model was manipulated to allow for a controlled method of altering the fetal blood saturation. A three-wavelength (730, 805, and ), single-separation, cw NIR instrument was employed to make transabdominal measurements of fetal oxygenation changes. The following sections describe in more detail the experimental protocol and instrumentation that was implemented. Next, the analytical solution used to estimate photon diffusion in this two-layer model is discussed thoroughly. Finally, the results present the extent of error propagation in the NIR calculations as several baseline optical properties are varied, specifically, the baseline fetal and maternal absorption coefficients, and the global reduced scattering coefficient. 2.Materials and Methods2.1.Animal PreparationThis animal study followed the National Institute of Health guidelines of the Institutional Animal Care and Use Committee at Cornell University, Ithaca, New York. This experiment was performed using a pregnant ewe model at a gestational age between (normal term ). The dam was anaesthetized with halothane and mechanically ventilated with 50% and 1.25% isoflurane. A midline abdominal incision exposed the uterus and a hysterotomy was performed to expose the fetal head.26 The fetal head was exteriorized from the amniotic sac. The left fetal brachial artery was catheterized for obtaining arterial blood samples and the right brachial artery was catheterized to monitor fetal blood pressure. The ears were sutured to the maternal abdomen such that the fetal head was directly under the maternal tissue, measured to be approximately thick. This procedure was done to eliminate the effect of amniotic fluid on the NIR measurements. A catheter was inserted through the maternal femoral artery with a balloon for aortic occlusion anterior to the common iliac artery. Occlusion was performed in a stepwise manner by incrementally filling the balloon with saline. This procedure induces fetal hypoxia by gradually limiting the amount of blood flow to the uterus and fetus, while not significantly affecting maternal oxygenation. A pulse oximeter was placed on the maternal ear to continuously measure arterial saturation and monitor maternal stability. Arterial blood samples were taken from the fetal brachial artery throughout the experiment. The fetal , Hb, pO2, pCO2, and pH values were measured by blood gas analysis using an OSM3 hemoximeter (Radiometer, Copenhagen) and an ABL605 blood gas analyzer (Radiometer, Copenhagen). 2.2.InstrumentationThe cw NIR spectroscopy probe consisted of one source position and one detector position. The optode separation was determined using a fast Fourier transform analysis of the signal component fluctuating at the fetal heart rate, which was simultaneously detected by an ultrasound fetal heart monitor placed on the maternal abdomen (Hewlett Packard m300). The highest signal-to-noise ratio was found at an optode separation of . The optical probe was placed on the maternal abdomen, such that the source and detector straddled the region above the fetal head. Three LEDs were implemented at 730, 805, and (Epitex, L735/805/850—40B32) and time-multiplexed. The intensities at each wavelength were detected by a photomultiplier (Hamamatsu Photosensor Module H6780). The signals were then filtered and sampled by an analog-to-digital converter (Real Time Devices, Inc. ADA2110). The data points were averaged at by the data acquisition software and saved for postprocessing. 2.3.Data Analysis2.3.1.The modelThe diffusion approximation of the radiative transport equation is the analytical model widely used to analyze photon migration in highly diffusive media. The diffusion approximation is based on the assumption that light propagating in highly scattering media is close to isotropic due to multiple scattering events. A large number of medical applications involving NIR spectroscopy or optical imaging have taken advantage of these approximations and have employed the diffusion equation to optically characterize and monitor the health status of biological tissue.27 In the diffusion approximation, the diffuse intensity moving in direction at position and at time may be expanded in spherical harmonics and expressed as the sum of two terms, one isotropic term proportional to the fluence rate and one term proportional to the diffused radiation flux:28 Here, is the energy density, and [cm] is the photon diffusion coefficient defined as , where is the reduced scattering coefficient of the medium. In the diffusion approximation, the directional flux is negligible compared to the isotropic term and can be omitted.29, 30 The detected signal is, therefore, considered approximately proportional to the energy density .The diffusion equation follows from this approximation and can be derived as where is the absorption coefficient, is the speed of light in the medium, and is the source. The Green’s function solution to the diffusion equation for an isotropic cw point light source in an infinite homogeneous medium iswhere is the distance from to the source.The infinite medium solution to the diffusion equation, however, does not accurately describe a situation in which the source and detector are placed on the surface of the tissue being investigated, as was done in this study. The necessary boundary condition must be implemented that accounts for the internal reflection encountered in a semi-infinite medium or half-space geometry. The extrapolated boundary approach was employed using the dipole method,31 wherein the fluence is nonzero on the boundary and set equal to zero at an extrapolated boundary located a distance outside the medium. In this dipole configuration a real light source is positioned beneath the surface at a distance , and a virtual image source is positioned directly above the surface at a distance . The effective diffuse Frenel reflectance for a relative index of refraction of (commonly assumed for air-tissue boundaries) was calculated as according to Haskell 30 The extrapolated boundary was then calculated as a function of the effective Fresnel reflectance such that This boundary condition was found by Kienle and Patterson32 to accurately resolve and from data generated with Monte Carlo to within 10% and 15%, respectively.The resulting Green’s function solution to the diffusion equation for a semi-infinite homogeneous medium is where is the distance from to the virtual image source.The volume being investigated in this study, however, was not an ideal homogeneous half-space. Rather it consisted of two layers, an upper maternal layer and a lower fetal layer. Although, it was assumed that the tissue scattering coefficient was uniform over both layers,22, 25 each layer could be characterized by its intrinsic absorption coefficient, which is a function of tissue blood volume and tissue blood oxygen saturation. In order to utilize the homogeneous Green’s function, a global absorption coefficient , taking into effect both the maternal and fetal baseline absorption coefficients, was used to represent a homogeneous absorption coefficient. It was assumed that fluctuations in absorption occurred within and uniformly over an entire layer and were defined with reference to , such that where is the variable absorption coefficient at position and at time .Therefore, measured changes in intensity were attributed to a fluctuating absorption coefficient in either one or both of the layers. The intensity measured by the detector was considered proportional to the energy density , which can be approximated as a linear function as described by:33 The weighting function was computed at each voxel in the entire volume, such thatThe expression in Eq. 7 represents the energy density propagating between the single source-detector pair in the absence of inhomogeneous absorption and can therefore be described by , such thatwhere represents the source power density, which in the case of this experiment was continuous wave .The measured energy density, proportional to energy density, fluctuated as we altered the fetal oxygenation. The NIR measurements were first smoothed with a boxcar average of 500 points, corresponding to a low-pass filter. This effectively removed arterial and respiratory fluctuations present in the data. The baseline energy density was assumed equal to the mean of the first 20 samples (approximately ). The natural logarithm of the transmission coefficient is then expressed as which can be further decomposed into two spatially resolved compartments,where the subscripts M and F represent the integral over voxel locations inside the maternal and fetal layers.In this experiment, it was assumed that the maternal absorption coefficient remains stable and that the fetal layer was the sole contributor to any absorption changes observed in the data. This assumption reduces Eq. 6 to It was further assumed that these absorption fluctuations occurred homogeneously over the entire fetal layer, which removes the position dependence from the fetal absorption coefficient and results in a simplified expression for the data:Here, the integral of over the fetal layer is essentially the partial differential pathlength (PDP).34A linear least-squares fit of a priori spectral information to the data in Eq. 8 was used to calculate the chromophore concentration changes [ and ] directly. The absolute fetal chromophore concentrations were calculated as follows: and . The initial fetal hemoglobin concentrations and were calculated from assumed fetal tissue blood volume (tHb) and fetal at baseline (Table 1 ). The fetal at each time point was then calculated simply as Table 1Summary of assumed baseline parameters. 2.3.2.Baseline optical propertiesThe measured chromophore concentration changes are essentially difference measurements from a known reference (baseline) point. Therefore, a NIR monitor must take an initial measurement during a stable, usually normoxic, state, during which the baseline absorption and scattering properties can be either measured (e.g., via FD or TRS methods) or safely assumed. The confidence of the NIR measurements, thus, relies heavily on the confidence of the chosen baseline properties. In this study, several baseline parameters were assumed in order to quantify the fetal chromophore concentration fluctuations measured in the data. These parameters were chosen based on values found in the literature15, 22, 25, 35, 36, 37, 38 and are described in Table 1. The maternal tHb, fetal tHb, maternal , and the global were varied over a range of values, since the literature indicates some intersubject variability. The error propagation due to uncertainty in these baseline parameters was analyzed. The best-fit baseline parameters were determined, using a downhill simplex method,39 by fitting the calculated fetal values to the measured fetal values (Table 1). The baseline fetal was not varied; it was assumed equal to the initial reading taken from blood gas analysis. In this experiment, the fetal was expected to remain in close approximation to the fetal . This assumption was founded on data published by Choe, 25 in which fetal and local venous saturation values were often close, if not overlapping, for normoxic and a range of hypoxic states. Generally, is modeled as a weighted average of and . However, the exact contributions in a subject are unknown and studies have demonstrated that they may not be fixed at all stages of hypoxia.40 Therefore, there may be some error due to correlating quantified NIR values to values, especially at low saturations (severe fetal hypoxia). However, in this study, this source of error has not been investigated; instead, the focus remains on the errors due to other baseline assumptions commonly made in quantifying tissue blood saturation. The global baseline absorption coefficient was calculated as a weighted combination of the maternal baseline absorption coefficient and the fetal baseline absorption coefficient . A wavelength-dependent background term representing fat and water40 was included in the absorption coefficient for each respective layer, such that . Since the extinction coefficients for fat and water are very similar and the concentration of fat is much less than that of water, . The errors due to the uncertainty in this background term were not considered in this study. The simplex routine assumed a 1:1 contribution ratio for the maternal and fetal absorption coefficients (a weight of 0.5 for each layer) in the determination of the best-fit baseline parameters. After the best-fit baseline values are chosen, the weight of each layer absorption coefficient was optimized using a least-mean-square algorithm, iterated over . The new weights were calculated based on the percent signal contributed from each layer, The new global baseline absorption coefficient was updated such thatand the change in squared error was calculated:The absorption coefficient weights were optimized when was minimized.3.Results and Discussion3.1.Hemodynamic Response in the Fetus Due to OcclusionRather than inflating the catheterized balloon with air, the balloon was incrementally filled with saline in order to observe a more gradual change in fetal chromophore concentrations. The balloon was filled in a step-wise manner, at a time, as arterial blood samples were taken from the fetus and the fetal values were noted. When fetal values reached a dangerous low, near 20%, the balloon was drained of saline to allow for fetal recovery. The changes in [Hb] and [HbO], calculated from the recorded NIR data, are shown in Fig. 1 . Fig. 1Fetal hemodynamic response due to occlusion. The solid line represents the average change in [HbO] over the course of the experiment and the dashed line represents the average change in [Hb] over time. The dotted line represents the volume of occlusion by filling a catheterized balloon with saline. The error bars represent the maximum variations in the calculated results as all of the parameters in Table 1 were altered simultaneously. 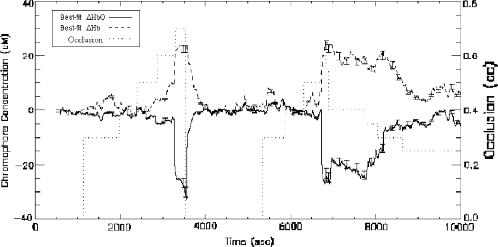 The fetus endured two trials of induced hypoxia and recovery. In the first trial, at of occlusion, a slight jump in fetal was observed followed by a return to baseline. At of occlusion, another increase in was observed. At occlusion, the fetal rose above baseline. At of occlusion, there was a steep rise in and a decrease in . At this point the fetal was measured to be close to 10% and the catheterized balloon was completely drained of all the saline. A return to baseline was immediately noticeable in both the and traces. The fetus needed approximately to fully recover (Fig. 1). At the start of the second trial, at of occlusion there was again a slight jump in followed by a return to baseline. At of occlusion, there was again an increase in . At of occlusion, there was a sharp increase in from baseline with an accompanying decrease in . At this point, the fetal was again measured to be close to 10%. In this second trial, instead of completely draining the balloon of saline, the volume of occlusion was decremented in a step-wise fashion. As occlusion was brought down to a volume of , the fell, while the fluctuated below baseline. As the volume of occlusion was reduced to , the began a more rapid return to baseline. At of occlusion, the also began a prompt return to baseline (Fig. 2 ). The ultrasound fetal heart rate monitor verified that the fetus remained alive throughout the entire experiment. Fig. 2Fetal calculated from NIR measurements. The diamonds represent the fetal measurements taken from blood gas analysis. The solid line is the average trace calculated the NIR data using the analytical semi-infinite model. The dotted line represents the volume of occlusion. The error bars represent the maximum variations in the calculated fetal St as a result of altering all of the parameters in Table 1 simultaneously. 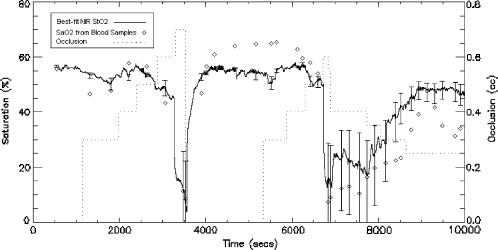 The calculated NIR curve also demonstrates a direct hemodynamic response due to the induced occlusion (Fig. 2). In the first hypoxic cycle, as the catheterized balloon reached a volume of , the fetal tissue blood saturation dropped sharply. In the second cycle, hypoxia was induced at an occlusion volume of . As the saline was withdrawn from the balloon, the NIR measurements returned to the tissue blood saturation baseline. However, the measurements overshoot the NIR measurements after the first recovery and undershoot the NIR measurements during the second recovery (Fig. 2). Figure 3 shows how the calculated correlates to the measurements. The relationship is not strongly linear over the whole range of measurements. However, without any fetal venous blood saturation measurements, it is unknown whether the calculated is linear with some weighted average of and . This weighted average may have also fluctuated during the experiment.40 Fig. 3Fractional error due to uncertainty in baseline optical properties. The triangles represent the fractional error in the calculated NIR results due to altering the maternal baseline absorption coefficient (i.e., the maternal tHb and parameters) over the specified range of reasonable values (Table 1). The squares represent the fractional error due to uncertainty in the baseline fetal absorption coefficient (in particular, the fetal tHb). The diamonds represent the fractional error due to uncertainty in . 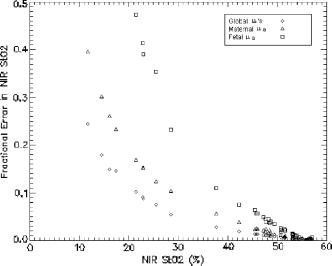 3.2.Error Propagation inThe NIR results were obviously most reliable while fetal oxygenation remained in close proximity to the fetal status at baseline. However, as fetal hypoxia was induced and fetal saturation levels fell, uncertainty in any of the assumed baseline parameters resulted in more variability in the calculated NIR measurements. In this study, the global reduced scattering coefficient, the baseline maternal absorption coefficient, and the baseline fetal absorption coefficient were independently varied over a range of possible values in order to investigate the error propagation in the calculated NIR measurements. The effect of error in each of the baseline parameters on the resulting calculation was measured as the fractional error (Fig. 3), given by: where and refer to the extrema of and represents the mean calculated at a specific point in time.The results of the error analysis show that uncertainty in the global reduced scattering coefficient, the baseline maternal absorption coefficient, and the baseline fetal absorption coefficient have similar effects on the NIR calculations. The error propagation due to the baseline maternal absorption coefficient was deduced by combining the effects of both the maternal tHb and the maternal baseline . The baseline fetal absorption coefficient was analyzed by varying the fetal tHb while the baseline fetal was held constant at the initial fetal reading (a likely saturation region). Above a best-fit of 40% (i.e., the calculated using the best-fit baseline parameters determined from the minimization routine), the fractional errors due to uncertainty in the baseline parameters are relatively low, between 0.1 and 0.2 (Fig. 3). It has been found in several animal studies, during which fetal arterial blood gas samples were drawn, that the “normal” range of fetal generally falls between 30 and 80%. (Studies have shown that fetal oxygen saturation below 30% is associated with declining fetal arterial pH.41) Therefore, these results are optimistic that fetal imbalance would most likely be detectable by the NIR . 3.3.Potential Sources of Error inSeveral broad assumptions were made about the baseline parameters considered in this study. First, it was assumed that the baseline parameters are restricted to a known range of values (Table 1), which was determined by values reported in the literature. However, it remains possible that these baseline values fall outside the expected range. Second, an important parameter which has not been considered here is the baseline fetal . The variation of this parameter is equivalent to varying , which essentially shifts the NIR curve. In this case, it was assumed that the fetal tissue blood saturation was approximately equal to the arterial saturation, and was fixed to the reading from the blood gas analysis. This may not always be the case, however, in an uncontrolled in vivo system. Knowledge of the true system geometry as well as a multidistance instrument are necessary to more accurately determine (a function of both fetal and maternal tHb and ), which is variable from subject to subject. The background absorption is another parameter that could be given more consideration in a further study. Here, it was assumed that the background absorption remains constant throughout the experiment. It was also assumed to be of equal weight in both the maternal and fetal layers. In actuality, the background absorption in the fetal layer could be due to a fat or water concentration different from that in the maternal layer. These concentrations may also change with variations in blood oxygenation.40 It was also assumed that the scattering coefficient remained constant throughout the experiment, over all stages of hypoxia. Other investigations have shown that the scattering coefficient does vary with oxygen saturation.40 This could lead to additional error, since any fluctuations in the data were considered solely absorptive. However, the changes in the absorption coefficient are much greater than those typically found in the scattering coefficient, so any error attributed to this assumption would most likely be relatively small. The analytical model used to analyze the NIR data was also founded on assumptions. In order to quantify the fluctuations in the data as fetal chromophore concentration changes, it was assumed that the maternal layer experienced no fluctuations [Eq. 12]. This assumption was based on the maternal arterial oxygen saturation values recorded by a pulse oximeter placed on the maternal ear. Yet, this does not ensure that no blood saturation changes occurred locally, in the maternal tissue visible to the source-detector probe. The feasibility of detecting the blood oxygen saturation of the fetal head, in utero, has been shown here. However, there is still much work to be done in the way of perfecting an instrument that would be used and trusted in a real clinical setting. One large concern arises from the fact that there is a layer of amniotic fluid between the fetal head and the maternal layer, characterized by a low absorption coefficient and a low scattering coefficient. This layer of amniotic fluid varies in thickness depending on the gestational age of the fetus and the fetal position. It has been shown that intervening amniotic fluid can significantly affect the photon migration path directly below the source. A large fraction of photons will be diverted around the fetal head before being detected at the surface, resulting in a smaller average absorption.22 A numerical model based on the radiative transport equation would more accurately simulate photon migration in cases where there is a nonuniform contact between the maternal abdomen and the fetal head. However, in cases of a late fetal gestational age, where the amniotic fluid layer is minimized, a simple two-layer diffusion model, such as that used in this study, will suffice. AcknowledgmentsThis research was supported in part by National Institutes of Health (NIH) grant HL061057, by a NIH-supported research resource grant, P41-RR02305, and by the National Heart, Lung, and Blood Institute, T32-HL07614. ReferencesD. James,
“Recent advances: fetal medicine,”
Br. Med. J., 316 1580
–1583
(1998). 0007-1447 Google Scholar
National Institute of Child Health,
“Electronic fetal heart rate monitoring: research guidelines for interpretation,”
Am. J. Obstet. Gynecol., 177
(6), 1385
–1390
(1997). 0002-9378 Google Scholar
K. B. Nelson,
J. M. Dambrosia,
T. Y. Ting, and
J. K. Grether,
“Uncertain value of electronic fetal monitoring in predicting cerebral palsy,”
N. Engl. J. Med., 334
(10), 613
–618
(1996). 0028-4793 Google Scholar
K. W. Murphy,
P. Johnson,
J. Moorcraft,
R. Pattinson,
V. Russell, and
A. Turnbull,
“Birth asphyxia and the intrapartum cardiotocograph,”
Br. J. Obstet. Gynaecol., 97
(6), 470
–479
(1990). 0306-5456 Google Scholar
W. W. Hay Jr.,
D. J. Rodden,
S. M. Collins,
D. L. Melara,
K. A. Hale, and
L. M. Fashaw,
“Reliability of conventional and new pulse oximetry in neonatal patients,”
J. Perinatol, 22
(5), 360
–366
(2002). 0743-8346 Google Scholar
B. Chance, Photon Migration in Tissue, Plenum, New York (1989). Google Scholar
F. F. Jobsis,
“Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters,”
Science, 198
(4323), 1264
–1267
(1977). 0036-8075 Google Scholar
P. L. Madsen and
N. H. Secher,
“Near-infrared oximetry of the brain,”
Prog. Neurobiol., 58
(6), 541
–560
(1999). 0301-0082 Google Scholar
Optical Tomography and Spectroscopy of Tissue: Theory, Instrumentation, Model, and Human Studies IIProc. SPIE, 2979
(1997)
(0277-786X) Google Scholar
A. Duncan,
J. H. Meek,
M. Clemence,
C. E. Elwell,
L. Tyszczuk, M. Cope, and
D. T. Delpy,
“Optical pathlength measurements on adult head, calf and forearm and the head of the newborn infant using phase resolved optical spectroscopy,”
Phys. Med. Biol., 40
(2), 295
–304
(1995). https://doi.org/10.1088/0031-9155/40/2/007 0031-9155 Google Scholar
D. T. Delpy and
M. Cope,
“Quantification in tissue near-infrared spectroscopy,”
Philos. Trans. R. Soc. London, Ser. B, 352 649
–659
(1997). https://doi.org/10.1098/rstb.1997.0046 0962-8436 Google Scholar
C. D. Kurth and
B. Uher,
“Cerebral hemoglobin and optical pathlength influence near-infrared spectroscopy measurement of cerebral oxygen saturation,”
Anesth. Analg. (Paris), 84
(6), 1297
–1305
(1997). 0003-3014 Google Scholar
S. R. Arridge,
M. Cope, and
D. T. Delpy,
“The theoretical basis for the determination of optical pathlengths in tissue: temporal and frequency analysis,”
Phys. Med. Biol., 37
(7), 1531
–1560
(1992). https://doi.org/10.1088/0031-9155/37/7/005 0031-9155 Google Scholar
E. M. Sevick,
B. Chance,
J. Leigh,
S. Nioka, and
M. Maris,
“Quantitation of time- and frequency-resolved optical spectra for the determination of tissue oxygenation,”
Anal. Biochem., 195
(2), 330
–351
(1991). https://doi.org/10.1016/0003-2697(91)90339-U 0003-2697 Google Scholar
J. C. Hebden,
A. Gibson,
R. M. Yusof,
N. Everdell,
E. M. Hillman,
D. T. Delpy,
S. R. Arridge,
T. Austin,
J. H. Meek, and
J. S. Wyatt,
“Three-dimensional optical tomography of the premature infant brain,”
Phys. Med. Biol., 47
(23), 4155
–4166
(2002). https://doi.org/10.1088/0031-9155/47/23/303 0031-9155 Google Scholar
Y. Hoshi,
“Functional near-infrared optical imaging: utility and limitations in human brain mapping,”
Psychophysiology, 40
(4), 511
–520
(2003). https://doi.org/10.1111/1469-8986.00053 0048-5772 Google Scholar
E. Keller,
A. Nadler,
H. Alkadhi,
S. S. Kollias,
Y. Yonekawa, P. Niederer,
“Noninvasive measurement of regional cerebral blood flow and regional cerebral blood volume by near-infrared spectroscopy and indocyanine green dye dilution,”
Neuroimage, 20
(2), 828
–839
(2003). 1053-8119 Google Scholar
S. L. Jacques,
N. Ramanujam,
G. Vishnoi,
R. Choe, and
B. Chance,
“Modeling photon transport in transabdominal fetal oximetry,”
J. Biomed. Opt., 5
(3), 277
–282
(2000). https://doi.org/10.1117/1.429996 1083-3668 Google Scholar
N. Ramanujam,
H. Long,
M. Rode,
I. Forouzan,
M. Morgan, B. Chance,
“Antepartum, transabdominal near infrared spectroscopy: feasibility of measuring photon migration through the fetal head in utero,”
J. Matern.-Fetal Med., 8
(6), 275
–288
(1999). https://doi.org/10.1002/(SICI)1520-6661(199911/12)8:6<275::AID-MFM8>3.0.CO;2-X 1057-0802 Google Scholar
A. Zourabian,
A. Siegel,
B. Chance,
N. Ramanujan,
M. Rode, D. A. Boas,
“Transabdominal monitoring of fetal arterial blood oxygenation using pulse oximetry,”
J. Biomed. Opt., 5
(4), 391
–405
(2000). https://doi.org/10.1117/1.1289359 1083-3668 Google Scholar
S. J. Matcher,
“Performance comparison of several published tissue near-infrared spectroscopy algorithms,”
Anal. Biochem., 227 54
–68
(1995). https://doi.org/10.1006/abio.1995.1252 0003-2697 Google Scholar
G. Vishnoi,
A. H. Hielscher,
N. Ramanujam, and
B. Chance,
“Photon migration through fetal head in utero using continuous wave, near-infrared spectroscopy: development and evaluation of experimental and numerical models,”
J. Biomed. Opt., 5
(2), 163
–172
(2000). https://doi.org/10.1117/1.429983 1083-3668 Google Scholar
B. W. Pogue,
K. D. Paulsen,
C. Abele, and
H. Kaufman,
“Calibration of near-infrared frequency-domain tissue spectroscopy for absolute absorption coefficient quantitation in neonatal head-simulating phantoms,”
J. Biomed. Opt., 5
(2), 185
–193
(2000). https://doi.org/10.1117/1.429985 1083-3668 Google Scholar
N. Ramanujam,
G. Vishnoi,
A. Hielscher,
M. Rode,
I. Forouzan, and
B. Chance,
“Photon migration through fetal head in utero using continuous wave, near infrared spectroscopy: clinical and experimental model studies,”
J. Biomed. Opt., 5
(2), 173
–184
(2000). https://doi.org/10.1117/1.429984 1083-3668 Google Scholar
R. Choe,
T. Durduran,
G. Yu,
M. J. Nijland,
B. Chance,
A. G. Yodh, and
N. Ramanujam,
“Transabdominal near infrared oximetry of hypoxic stress in fetal sheep brain in utero,”
Proc. Natl. Acad. Sci. U.S.A., 100
(22), 12950
–12954
(2003). https://doi.org/10.1073/pnas.1735462100 0027-8424 Google Scholar
M. J. Nijland,
U. Shankar,
V. Iyer, and
M. G. Ross,
“Assessment of fetal scalp oxygen saturation determination in the sheep by transmission pulse oximetry,”
Am. J. Obstet. Gynecol., 183
(6), 1549
–1553
(2000). 0002-9378 Google Scholar
Optical Tomography, Photon Migration, and Spectroscopy of Tissue and Model Media: Theory, Human Studies, and Instrumentation, Parts 1 and 2Proc. SPIE, 2389
(1995)
(0277-786X) Google Scholar
A. Ishimaru, Wave Propagation and Scattering in Random Media, Academic Press, New York (1978). Google Scholar
T. Nakai,
G. Nishimura, and
K. Yamamoto,
“Expression of optical diffusion coefficient in high-absorption turbid media,”
Electron. Commun. Jpn., Part 2: Electron., 81
(11), 34
–41
(1998). 8756-663X Google Scholar
R. C. Haskell,
L. O. Svaasand,
T. T. Tsay,
T. C. Feng,
M. S. McAdams, and
B. J. Tromberg,
“Boundary conditions for the diffusion equation in radiative transfer,”
J. Opt. Soc. Am. A, 11
(10), 2727
–2741
(1994). 0740-3232 Google Scholar
T. J. Farrell,
M. S. Patterson, and
B. Wilson,
“A diffusion theory model of spatially resolved, steady-state diffuse reflectance for the noninvasive determination of tissue optical properties in vivo,”
Med. Phys., 19
(4), 879
–888
(1992). https://doi.org/10.1118/1.596777 0094-2405 Google Scholar
A. Kienle and
M. S. Patterson,
“Improved solutions of the steady-state and the time-resolved diffusion equations for reflectance from a semi-infinite turbid medium,”
J. Opt. Soc. Am. A, 14
(1), 246
–254
(1997). 0740-3232 Google Scholar
J. S. Souris,
“Diffusing wave emission tomography in highly-scattering systems: a dissertation in biochemistry and molecular biophysics,”
(1999) Google Scholar
M. Hiraoka,
M. Firbank,
M. Essenpreis,
M. Cope,
S. R. Arridge, P. van der Zee, and
D. T. Delpy,
“A Monte Carlo investigation of optical pathlength in inhomogeneous tissue and its application to near-infrared spectroscopy,”
Phys. Med. Biol., 38
(12), 1859
–1876
(1993). https://doi.org/10.1088/0031-9155/38/12/011 0031-9155 Google Scholar
M. Cope,
“The application of near infrared spectroscopy to non-invasive monitoring of cerebral oxygenation in the newborn infant,”
(1991) Google Scholar
A. Gibson,
R. M. Yusof,
H. Dehghani,
J. Riley,
N. Everdell,
R. Richards,
J. C. Hebden,
M. Schweiger,
S. R. Arridge, and
D. T. Delpy,
“Optical tomography of a realistic neonatal head phantom,”
Appl. Opt., 42
(16), 3109
–3116
(2003). 0003-6935 Google Scholar
P. Taroni,
A. Pifferi,
A. Torricelli,
D. Comelli, and
R. Cubeddu,
“In vivo absorption and scattering spectroscopy of biological tissues,”
Photochem. Photobiol. Sci., 2
(2), 124
–129
(2003). 1474-905X Google Scholar
J. S. Matcher,
M. Cope, and
D. T. Delpy,
“In vivo measurements of the wavelength dependence of tissue-scattering coefficients between 760 and measured with time-resolved spectroscopy,”
Appl. Opt., 36 386
–396
(1997). 0003-6935 Google Scholar
W. H. Press and Numerical Recipes Software (Firm, Numerical Recipes in C, Cambridge University Press, Cambridge, England, New York (1993). Google Scholar
D. M. Hueber,
M. A. Franceschini,
H. Y. Ma,
Q. Zhang,
J. R. Ballesteros,
S. Fantini,
D. Wallace,
V. Ntziachristos, and
B. Chance,
“Non-invasive and quantitative near-infrared hemoglobin spectrometry in the piglet brain during hypoxic stress, using a frequency-domain multidistance instrument,”
Phys. Med. Biol., 46
(1), 41
–62
(2001). https://doi.org/10.1088/0031-9155/46/1/304 0031-9155 Google Scholar
D. M. Gorenberg,
C. Pattillo,
P. Hendi,
P. J. Rumney, and
T. J. Garite,
“Fetal pulse oximetry: correlation between oxygen desaturation, duration, and frequency and neonatal outcomes,”
Am. J. Obstet. Gynecol., 189
(1), 136
–138
(2003). 0002-9378 Google Scholar
|



