
|
|
1.IntroductionOtosclerosis is the abnormal growth of bone in the otic capsule. It often results in fixation of the stapes footplate to the oval window, resulting in conductive hearing loss.1 Treatment is usually by a stapedotomy—a perforation is created in the stapes footplate, into which a piston-like prosthetic device is inserted and coupled to the incus.2 Surgical procedures of the stapes and middle ear require precision, while minimizing damage to sensitive inner ear structures and the facial nerve. A high-power laser is commonly used to fenestrate the stapes. Numerous lasers have been used3 for this procedure, including argon , KTP Nd:YAG , Er:YAG , and . However, none of these lasers are ideal for performing stapedotomy. For example, the visible light of argon and KTP lasers is weakly absorbed by the perilymph, and therefore penetrates to the sensitive hearing and balance organs of the inner ear. The IR light of Er:YAG and is more readily absorbed, but short high-energy pulses result in large pressure transients, which could cause acoustic trauma. An ideal laser system for middle ear surgery would have thermal and stress confinement. Femtosecond (fs) laser pulse ablation occurs with minimal thermal or mechanical injury. Tightly focused high-intensity ultrashort pulses ionize material to produce a mixture of free electrons and ions, termed plasma, in the focal point of the laser beam. Laser energy is then absorbed by the plasma, so that the process is only weakly dependent on the tissue characteristics. Ablation is very precise because it is confined to the region of ionization. There is little or no heating outside the targeted area because ablation occurs more rapidly than thermal diffusion.4 Ultrashort laser pulses have been shown to effectively ablate bone and hard tissue.5, 6, 7, 8, 9, 10 This study evaluates the ablation of ossicular bone with a femtosecond laser, commonly used in LASIK eye surgery.11 2.Materials and MethodsA Model I Intralase FS laser (AMO Corp, Santa Ana, California), commonly used for LASIK eye surgery, was used to irradiate the bone. The laser produces , pulses of up with a repetition rate of . The diameter at the focal point of the laser beam in air is approximately (as quoted by Intralase specifications). Computer-controlled mirrors scanned the beam in a spiral pattern of increasing diameter with an accuracy of . The planar glass window of the delivery system was removed because vaporized bone collected on the lens and shielded the sample from the laser. The focusing optics were not modified, and it is assumed the optical properties of the beam were not significantly altered by removing the glass window. The focus of the laser beam was aligned with the surface of the sample by adjusting the height of the sample relative to the laser output. The focus was determined to be coincident with the surface at the point at which bright visible plasma was observed. Porcine otic capsule bone was ablated to emulate the stapedotomy operation. The otic capsule surrounds the membranous labyrinth of the inner ear and provides a hard bony casing to protect the organs of hearing and balance. The stapes footplate is derived from the otic capsule, so they are histologically and embryologically similar.12 The otic capsule was removed from the temporal bones of fresh pig skulls, obtained from a large regional packing company (Clougherty Packing LLC, Los Angeles, California). The skulls were divided in a midsaggital plane. The brain was carefully removed to expose the otic capsule that lies along the middle section of the petrous ridge. The otic capsule in the domestic pig is separate from the rest of the temporal bone and is easily pried loose with a narrow osteotome. The entire otic capsule was removed intact and is approximately in size. A low-speed microstructural saw with a diamond wafering blade (Buehler, Lake Bluff, Illinois) was used to machine the bone into slices approximately thick, to represent the stapes. Temporal bones were obtained from cadavers through the Willed Body Program at the University of California, Irvine. Each specimen was examined for otosclerosis, other disease processes and erosion of the stapes. Access to the middle ear was acquired via a tympanomeatal flap. The incudostapedial joint was visualized and carefully dislocated. The stapedial tendon was sectioned, and the stapes was removed in its entirety, maintaining the integrity of the stapes superstructure and footplate. Figure 1 shows a model vestibule, which grossly conforms to volumetric measurements from temporal bone atlases. It was constructed by drilling a -diam hole through the center of an acrylic block. Three small ports ( in diameter) were drilled from the side of the block into the cavity to enable the insertion of a thermocouple. The ports were positioned 1.0, 3.0, and below the upper surface of the chamber. The chamber was filled with water to mimic perilymph. For further details see Ref. 13. A type E, beaded, 24AWG glass braid insulated wire thermocouple (Omega Co., Stamford, Connecticut) connected to an integrated signal conditioning data acquisition module (NI-USB 9211A, National Instruments, Austin, Texas) was used to measure the temperature in the model vestibule. Photomechanical stress was measured with a piezoelectric fluoropolymer film (PVDF) transducer (SDT series, Measurement Specialties, Inc., Hampton, Virgenia) connected to a data acquisition module (NI-USB 6211, National Instruments, Austin, Texas). The piezo film produces voltage in proportion to compressive or tensile mechanical stress (piezo stress constant, ). Ultrasound gel (Aquasonic 100, Parker Laboratories, Inc., Fairfield, New Jersey) was placed between the PVDF and the bone specimen to minimize acoustic reflections. Acoustic events were recorded with a unidirectional dynamic microphone (frequency response: , impedance: , sensitivity: , RadioShack) from the bone sample. Optical coherence tomography (OCT) of the ablation craters was carried out with a Niris Imaging System (Imalux Corporation, Cleveland, Ohio). It has a lateral resolution of and a depth resolution of . Microscopy was performed with a Philips XL30 Scanning Electron Microscope (FEI, Hillsboro, Oregon). Samples were fixed in osmium tetraoxide, dehydrated, and sputter coated with gold prior to imaging with the scanning electron microscope (SEM). 3.Results3.1.Porcine Otic CapsuleIrradiation of the otic capsule slices resulted in a bright plasma on the surface of the bone. The threshold for a visible plasma was (approximately ). A scan spiral of diameter took , while took . The time to complete the scan increased quadratically with scan diameter. Figure 2 shows ablation from a femtosecond beam of pulse energy with a separation of between each scan position, scanned over an area in diameter. It is compared to ablation by 10 pulses from an Ultrafine Er:YAG laser (Coherent Inc, Santa Clara, California). Measurement by OCT found the crater from the femtosecond laser to be deep. No evidence of thermal damage or charring was observed when ablating with the femtosecond laser. The crater base and walls of the femtosecond ablation are considerably smoother and better defined than those created by Er:YAG, as shown in Fig. 2. The OCT images [Figs. 2b and 2f] show that the femtosecond laser produces perpendicular crater walls and a flat base, compared to the ErYAG crater that has sloping walls and a base that is deeper at the periphery than in the center. Fig. 2Otic capsule bone ablated with femtosecond (a) to (d) and Er:YAG (e) to (h) lasers: (a) and (e), light microscopy; (b) and (f), OCT; (c) and (g), ; and (d) and (h), . 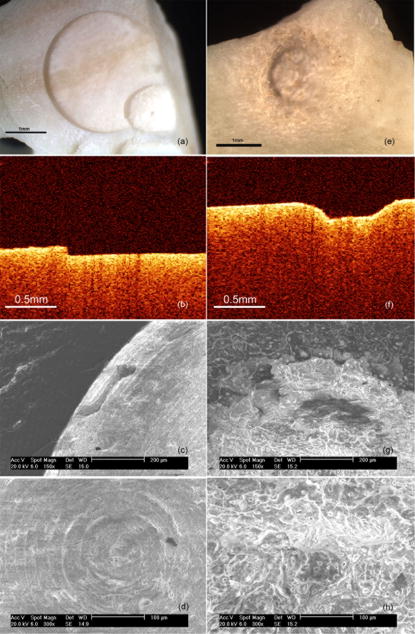 The SEM images of the femtosecond crater edge [Fig. 2c] confirm that the ablated area ends abruptly, with no damage to the surrounding bone. In comparison, the Er:YAG crater [Fig. 2g] has no clear boundary—a region of approximately of damaged tissue encircles the crater. Figures 2d and 2h show the base of the femtosecond and Er:YAG craters, respectively. The rings of the scanned femtosecond beam are evident in Fig. 2d. The surface is much smoother than the Er:YAG base [Fig. 2h]. Figure 3 shows the temperature increase on the back surface of a slice of otic capsule for spiral patterns of different diameters. Every 10th data point was sampled for clarity. The thermocouple was in direct contact with the bone in the center of the spiral. The beam diameter was with separation between consecutive delivery positions. The energy per pulse was . The temperature growth and decay follow the same trend, but the maximum temperature increase is greater for larger spiral diameters. Fig. 3Temperature increase on the back surface of a slice of otic capsule for spiral patterns of different diameters.  Figure 4 shows the temperature increase on the rear surface of a thick otic capsule slice for pulse energies 10, 8, 6, 4, 2, and in a scan diameter. The beam diameter was , with a separation of . The maximum temperature increase is linear with respect to pulse energy, as shown in Fig. 5 . Fig. 4Temperature increase on the rear surface of a otic capsule slice for different pulse energies.  Figure 6 shows how the temperature increase in the model ear below the stapes for a pulse scanned over . The temperature increase 3 and below the stapes in the model ear was negligible. Any photoacoustic stress or sound was too small or out of the range of the detectors to record. By comparison a , pulse (parameters used for efficient ablation) from an Er:YAG laser generates14 a peak stress of . 3.2.Human StapesFigure 7 shows a human stapes with a -diam perforation in the footplate created with the femtosecond laser. A beam focused to ablated the footplate. The SEM image confirms that the perforation is a smooth cut with well-defined edges. 4.DiscussionThe findings of precise ablation of otic capsule bone were duplicated in the human stapes. The well-defined ablation crater and the lack of damage to surrounding tissue created by the femtosecond laser will ensure a potentially smoother fit for prosthetic devices used in stapedotomy. The small beam size coupled with computerized scanning of the femtosecond device means precise perforations of any shape can be obtained. The temperature increases of the order of associated with beams are well tolerated in middle ear surgery. Noyes found that a temperature increase of did not impair hair cell function in the rabbit cochlea.15 Repetition of the procedure to achieve the desired ablation depth may be required, but this will result in only a modest accumulation of heat. The heat generated will not be easily transported to the sensitive inner ear organs, as evidenced by Fig. 6. One millimeter into the “perilymph,” the temperature increase is less than , and there is no noticeable temperature increase beyond the stapes. During ultra-short-pulse laser ablation, electrons are transferred to the conduction band of dielectric materials by multiphoton ionization and other nonlinear effects. Relaxation occurs through electron-phonon coupling (generation of heat) or by radiative decay (fluorescence). The absorbed energy is transferred to breaking of the material bonds, formation of excited fragments, and expulsion of the resulting vapors. A small part of the laser energy is transferred to the bulk through convective heating of the emerging plasma plume, electron-phonon relaxation without defragmentation and reabsorption of fluorescent radiation. This remaining energy heats the surrounding tissue. By observing the thermal effects in the irradiated tissue it is possible to estimate the proportion of the laser energy that contributes to heating the material. The temperature from a time-dependent point source, at distances much greater than the size of the beam, can be approximated by where is the fraction of the laser energy that contributes to heating, is the heat source, is the conductivity, is the diffusivity, and is the distance from the source.13 The spiral scanning pattern has been simplified to a ring of increasing radius such that . Solving Eq. 1 and fitting to the experimentally measured temperature, was found to be 0.05. This is in good agreement with Neev who found to be 0.07 for dentin irradiated with a femtosecond laser.16 Figure 8 compares the temperature increase measured on the rear surface of a -thick bone slice irradiated with laser pulses scanned over a radius, and the temperature predicted by Eq. 1.Fig. 8Comparison of the temperature increase measured on the rear surface of a -thick bone slice irradiated with laser pulses scanned over a radius, and the temperature predicted by Eq. 1. 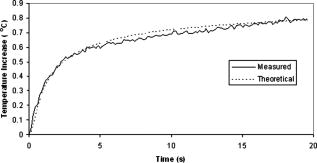 This model also predicts a linear increase in temperature with pulse energy, in agreement with the measured trend shown in Fig. 5. The thermoelastic expansion of the high-energy density plasma and the recoil stress from the ejection of ablated material should generate mechanical stresses. However, no pressure wave or acoustic events were measured during ablation. This may be because the short time periods involved result in shock waves of very high frequency (∼gigahertz). Such high frequencies do not propagate well in tissue, and the energy is reabsorbed within a few micrometers.17 This observation is in agreement with results obtained with optical measurements indicating the short (10- to ) decay of shockwaves generated with femtosecond photodisruption in water and in corneal tissue.18 Neev also reported negligible acoustic events when ablating hard tissue with an ultra-short-pulse laser.19 This offers femtosecond ablation a significant advantage over Er:YAG, which is characterized by a loud popping. This is especially important for middle ear surgery where acoustic events could cause trauma to sensitive inner ear organs. Future studies will include in vitro measurements of temperature in human bone and in vivo studies of femtosecond laser use within the middle ear of animals and humans. A system is currently being developed to deliver this novel use of the femtosecond laser to the human temporal bone. 5.ConclusionA femtosecond laser, normally used for LASIK eye surgery, was used to ablate porcine otic capsule bone and human stapes bones. Optical microscopy, OCT, and scanning electron microscopy show the ablation craters to be smooth and precise. Thermal side effects were shown to be minimal, and acoustic and mechanical events were negligible. These characteristics indicate that the Intralase FS device could have applications in middle ear surgery, including human stapedotomy. AcknowledgmentsThe authors would like to thank Lih-Huei Liaw, MS, for her assistance with the microscopy. ReferencesH. F. Schuknecht, Pathology of the Ear,
(1974) Google Scholar
U. Fisch,
“Stapedotomy versus stapedectomy,”
Am. J. Otol., 4
(2), 112
–117
(1982). 0192-9763 Google Scholar
M. Frenz,
“Physical characteristics of various lasers used in stapes surgery,”
Adv. Oto-Rhino-Laryngol., 65 237
–249
(2007). https://doi.org/10.1159/000098838 0065-3071 Google Scholar
A. Vogel and V. Venugopalan,
“Mechanisms of pulsed laser ablation of biological tissues,”
Chem. Rev. (Washington, D.C.), 103
(2), 577
–644
(2003). https://doi.org/10.1126/science.301.5633.577a 0009-2665 Google Scholar
B. Girard, D. Yu, M. R. Armstrong, B. C. Wilson, C. M. L. Clokie, and R. J. D. Miller,
“Effects of femtosecond laser irradiation on osseous tissues,”
Lasers Surg. Med., 39
(3), 273
–285
(2007). https://doi.org/10.1002/lsm.20466 0196-8092 Google Scholar
W. B. Armstrong, J. A. Neev, L. B. Da Silva, A. M. Rubenchik, and B. C. Stuart,
“Ultrashort pulse laser ossicular ablation and stapedotomy in cadaveric bone,”
Lasers Surg. Med., 30
(3), 216
–220
(2002). https://doi.org/10.1002/lsm.10034 0196-8092 Google Scholar
J. Neev, J. S. Nelson, M. Critelli, J. L. McCullough, E. Cheung, W. A. Carrasco, A. M. Rubenchik, L. B. D. Silva, M. D. Perry, and B. C. Stuart,
“Ablation of human nail by pulsed lasers,”
Lasers Surg. Med., 21
(2), 186
–192
(1997). https://doi.org/10.1002/(SICI)1096-9101(1997)21:2<186::AID-LSM10>3.0.CO;2-D 0196-8092 Google Scholar
B. Schwab, D. Hagner, J. Bornemann, and R. Heermann,
“The use of femtosecond technology in Otosurgery,”
Femtosecond Technology for Technical and Medical Applications, 211
–226 ,
(2004). Google Scholar
Y. Liu and M. Niemz,
“Ablation of femural bone with femtosecond laser pulses—a feasibility study,”
Lasers Med. Sci., 22
(3), 171
–174
(2007). https://doi.org/10.1007/s10103-006-0424-8 0268-8921 Google Scholar
J. Ilgner, M. Wehner, J. Lorenzen, M. Bovi, and M. Westhofen,
“Morphological effects of nanosecond- and femtosecond-pulsed laser ablation on human middle ear ossicles,”
J. Biomed. Opt., 11
(1), 014004
(2006). https://doi.org/10.1117/1.2166432 1083-3668 Google Scholar
P. S. Binder,
“Flap dimensions created with the IntraLase FS laser,”
J. Cataract Refractive Surg., 30
(1), 26
–32
(2004). https://doi.org/10.1016/S0886-3350(03)00578-9 0886-3350 Google Scholar
B. Wong, L.-H. Liaw, J. Neev, and M. Berns,
“Scanning electron microscopy of otic capsule and calvarial bone ablated by a holmium-YAG laser,”
Lasers Med. Sci., 9
(4), 249
–260
(1994). https://doi.org/10.1007/BF02593887 0268-8921 Google Scholar
B. J. F. Wong, J. P. Lee, M. R. Dickinson, J. Neev, and L. O. Svaasand,
“Photothermal-induced temperature changes in a model inner ear: A comparison of visible, infrared, and ultraviolet lasers,”
IEEE J. Sel. Top. Quantum Electron., 2
(4), 951
–958
(1996). https://doi.org/10.1109/2944.577321 1077-260X Google Scholar
R. G. McCaughey, B. J. F. Wong, J. Tafoya, Y. Sun, and R. Jain,
“Compact infrared laser for stapedotomy,”
Proc. SPIE, 6842 68421E
(2008). https://doi.org/10.1117/12.771759 0277-786X Google Scholar
W. S. Noyes, T. V. McCaffrey, D. A. Fabry, M. S. Robinette, and V. J. Suman,
“Effect of temperature elevation on rabbit cochlear function as measured by distortion-product otoacoustic emissions,”
Otolaryngol.-Head Neck Surg., 115
(6), 548
–552
(1996). https://doi.org/10.1016/S0194-5998(96)70009-8 0194-5998 Google Scholar
J. Neev, L. B. Da Silva, M. D. Feit, M. D. Perry, A. M. Rubenchik, and B. C. Stuart,
“Ultrashort pulse lasers for hard tissue ablation,”
IEEE J. Sel. Top. Quantum Electron., 2
(4), 790
–800
(1996). https://doi.org/10.1109/2944.577301 1077-260X Google Scholar
A. A. Oraevsky, L. B. Da Silva, A. M. Rubenchik, M. D. Feit, M. E. Glinsky, M. D. Perry, B. M. Mammini, W. I. Small, and B. C. Stuart,
“Plasma mediated ablation of biological tissues with nanosecond-to-femtosecond laser pulses: relative role of linear and nonlinear absorption,”
IEEE J. Sel. Top. Quantum Electron., 2
(4), 801
–809
(1996). https://doi.org/10.1109/2944.577302 1077-260X Google Scholar
T. Juhasz, G. A. Kastis, C. Suárez, Z. Bor, and W. E. Bron,
“Time-resolved observations of shock waves and cavitation bubbles generated by femtosecond laser pulses in corneal tissue and water,”
Lasers Surg. Med., 19
(1), 23
–31
(1996). https://doi.org/10.1002/(SICI)1096-9101(1996)19:1<23::AID-LSM4>3.0.CO;2-S 0196-8092 Google Scholar
J. Neev, D. S. Huynh, W. A. Carrasco, P. B. B. Wilder-Smith, L. B. Da Silva, M. D. Feit, M. D. Perry, A. M. Rubenchik, and B. C. Stuart,
“Thermal and noise level characteristics of hard dental tissue ablation with pulse laser,”
Proc. SPIE, 2672 262
–271
(1996). https://doi.org/10.1117/12.238776 0277-786X Google Scholar
|







