|
|
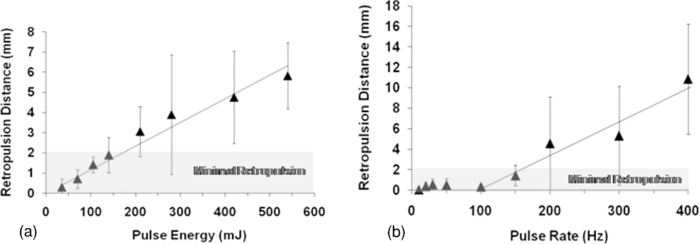
1.IntroductionKidney stone disease is a common and costly disorder in the United States. Up to 12% of males and 7% of females are affected during their lifetime.1 Estimates of annual costs to the national health care system reach $5.3 billion. Each year, over 3 million patient visits to health care providers occur with over 500,000 treatments in emergency rooms for kidney stone problems.2 Furthermore, recent global warming studies predict significant climate-related increases in stone disease in the coming decades, including a 10% increase in prevalence and 25% increase in costs.3 A significant percentage of kidney stone presentations require surgical intervention. Laser lithotripsy, predominantly via advanced ureteroscopy, has become a major technique for the minimally invasive surgical destruction of ureteral and kidney stones. For small to moderate sized or multiple urinary stones, this technology is the preferred surgical option over even extracorporeal shock wave lithotripsy in many centers in this country. Maximal clinical efficiency of laser lithotripsy is important to decrease operative time, surgical risk, and costs. The rate of stone destruction, or ablation rate, is a significant measure of efficiency. Laser energy tends to propel stones backward (resulting in retropulsion) from the optical fiber tip unless the stone is fixed or impacted by surrounding tissues within the ureter or kidney. Retropulsion is a clinically significant phenomenon, as it causes the surgeon to “chase” the stone, resulting in a decrease in ablation efficiency and increase in surgical time. Less retropulsion would be a desirable feature of a laser lithotripter. The solid-state holmium:YAG laser (Ho:YAG) has become the principal laser lithotripter in clinical use over the past 15 years. However, our research group has been studying the thulium fiber laser (TFL) as a potential alternative lithotripter.4, 5, 6, 7 The TFL has several potential advantages over the Ho:YAG laser. The TFL wavelength (λ = 1908 nm) more closely matches a high-temperature water absorption peak in tissue than the Ho:YAG wavelength (λ = 2120),8 which may lead to improved stone ablation. The excellent TFL spatial beam profile also allows coupling of higher laser power into smaller optical fibers. For intricate lithotripsy procedures that require extreme flexion of the miniature ureteroscope (e.g., into the lower pole of the kidney), a smaller fiber permits greater flexibility of the instrument. The smaller fiber also permits increased irrigation through the minute working channel within the instrument, improving visibility and, hence, safety.5, 6 Although the clinical flashlamp-pumped Ho:YAG laser is capable of operating at high pulse energies, efficient operation is limited to relatively low pulse repetition rates (∼10 Hz) during lithotripsy. The Ho:YAG laser is also associated with considerable retropulsion, as described above. On the contrary, while the experimental diode-pumped TFL is limited to low pulse energies, it is capable of operating efficiently at high pulse rates (up to 1000 Hz). The purpose of this study is to compare the performance of the two different laser lithotripters to determine which operational mode is most preferable for lithotripsy, Ho:YAG (high pulse energy and low pulse rate) or TFL (low pulse energy and high pulse rate). Human calcium oxalate monohydrate stones were used in this study because the majority of stones (∼80%) are of a calcium-based composition.9 The ablation thresholds, ablation rates, and retropulsion effects were measured and compared for each lithotripter. 2.Methods2.1.Stone Sample PreparationHuman calcium oxalate monohydrate (COM) urinary stone samples with masses of 200 to 1100 mg and of purity greater than 95% were obtained from two stone analysis laboratories (Louis C. Herring & Co., Orlando, Florida and Labcorp, Oklahoma City, Oklahoma) and used for the ablation threshold and ablation rate studies. Spherical plaster-of-Paris stone phantoms having approximately the same size (6-mm-diameter) and density as COM stones were created using a mold and then used for the stone retropulsion studies as a standard model for providing more reproducible results than the irregularly shaped COM stones. A minimum of five stone samples were used for each set of laser parameters and the mean ± standard deviation was plotted for each data point. 2.2.Laser ParametersA clinical holmium:YAG laser (TwoPointOne XE, Coherent, Santa Clara, California) was operated with a wavelength of 2120 nm, variable pulse energies of 30 to 550 mJ, 350-μs pulse duration, and a pulse rate of 10 Hz. For comparison, an experimental thulium fiber laser (TLR 110–1908, IPG Photonics, Inc., Oxford, Massachusetts) was externally modulated with a function generator (Model DS345, Stanford Research Systems, Sunnyvale, California) to operate in pulsed mode with a wavelength of 1908 nm, pulse energies of 5 to 35 mJ, 500-μs pulse duration, and pulse rates of 10 to 400 Hz. 2.3.Ablation ThresholdsThe ablation threshold, defined as the lowest incident fluence at which stone material is removed, was measured for human COM stones after lithotripsy with the Ho:YAG and TFL. Stone samples were held fixed and submerged in a saline bath for the studies. For each laser, the pulse rate was fixed at 10 Hz and a fixed number of 6000 pulses were delivered through 200-μm-core optical fibers (BFL22–200, Thorlabs, Newton, New Jersey) in contact mode with the stone. The pulse energy was escalated in small increments until stone mass loss could be measured, using an analytical balance (AB54-S, Mettler-Toledo, Switzerland). Total mass loss measurements less than 1 mg, after delivery of a total of 6000 pulses, were considered to be within experimental error and negligible. Furthermore, when divided by a total of 6000 pulses, this value translates into a mass loss of less than 1 μg per laser pulse, which is not directly observable, and is negligible compared to typical mass removal rates of 100's μg/pulse typically produced when the Ho:YAG laser is operated at clinical settings. The ablation threshold was then determined by plotting mass loss (mg) versus fluence (J/cm2) with a linear fit to the data. The x-intercept of this fit determined the ablation threshold value. 2.4.Ablation RatesHo:YAG laser lithotripsy at a fixed pulse rate of 10 Hz and pulse energies of 30 to 165 mJ was compared to TFL at a fixed pulse energy of 35 mJ and pulse rates of 10 to 100 Hz. Silica optical fibers with 200-μm-core diameter delivered the laser radiation in contact mode to human COM stones submerged and held fixed in a saline bath. After 6000 pulses, stone mass loss was measured and average stone vaporization rates (μg/s) were plotted. 2.5.Retropulsion StudiesLaser energy was delivered through 270-μm optical fibers (Olympus Gyrus ACMI, Southborough, Massachusetts) in contact mode with 6-mm-diameter Plaster-of-Paris (PoP) stone phantoms, submerged in a saline bath (Fig. 1). A rigid ureteroscope (9.5-Fr ID, Karl Storz, Germany) attached to a light source (X7000, Stryker Endoscopy, San Jose, California), camera (1188HD, Stryker), and monitor were used to accurately position the optical fiber tip so it was perpendicular to, centered on, and in contact with the PoP stone phantom prior to irradiation. Stone retropulsion distance was measured for each set of laser parameters for a fixed total energy (42 J) delivered to the stone. Fig. 1Experimental setup for studying retropulsion during holmium:YAG and thulium fiber laser lithotripsy using plaster-of-Paris stone phantoms. A rigid ureteroscope attached to a light source, camera, and monitor was used to accurately position the optical fiber tip so it was perpendicular to, centered on, and in contact with the stone prior to irradiation.  3.Results3.1.Ablation ThresholdsTo determine the ablation thresholds for the Ho:YAG and TFL wavelengths, the data was plotted as mass loss versus fluence (Fig. 2). Both graphs show a highly linear fit to the data points, with the slope giving a measurement of the ablation rate and the x-intercept providing the ablation threshold. The COM stone ablation threshold for the Ho:YAG and TFL measured 82.6 J/cm2 and 20.8 J/cm2, respectively. The ablation rates (slopes of linear fits) shown in Fig. 2 were approximately equivalent. Fig. 2Determination of the ablation threshold for human calcium oxalate monohydrate stones in terms of mass loss after delivery of 6000 laser pulses. (a) The ablation threshold for the holmium:YAG laser wavelength of 2120 nm measured approximately 82.6 J/cm2. (b) The ablation threshold for the thulium fiber laser wavelength of 1908 nm measured 20.8 J/cm2.  3.2.Ablation RatesThe data provided in Fig. 2 was obtained only at relatively low pulse energies and fluencies close to the ablation threshold for COM stones and only at a low pulse rate of 10 Hz for both lasers. However, the Ho:YAG laser is not limited to operation at low pulse energies and the TFL is not limited to operation at low pulse rates. Therefore, another study was also conducted to compare optimal operation of the Ho:YAG laser at high pulse energies (but low pulse rate of 10 Hz) and TFL at high pulse rates (but low pulse energy of 35 mJ). The results of this study are shown in Fig. 3. The Ho:YAG ablation rate linearly increased with pulse energy as expected [Fig. 3a], resulting in a COM stone vaporization rate of 100 μg/s at a pulse energy of about 165 mJ. On the contrary, although the TFL ablation rate also continued to increase with increasing pulse rate, the rate of increase was not linear as shown in Fig. 3b. Instead, an increase in pulse rate from 10 to 100 Hz did not result in an anticipated ablation rate increase of 10-fold, but rather only a 5-fold increase from 28 to 140 μg/s. 3.3.Retropulsion StudiesFigure 4 shows the amount of retropulsion measured for plaster-of-Paris stone phantoms using the Ho:YAG and TFL. Retropulsion with the holmium laser linearly increased with increasing pulse energy. Retropulsion with the TFL was minimal at pulse rates less than approximately 150 Hz then rapidly increased with higher pulse rates. For the purposes of this study, minimal retropulsion was defined as a retropulsion distance of less than 2 mm. This criteria would imply that Ho:YAG laser settings of greater than 175 mJ at 10 Hz with a 270-μm fiber results in significant retropulsion. TFL lithotripsy at pulse rates greater than 150 Hz at 35 mJ resulted in significant retropulsion as well. 4.Discussion4.1.Ablation ThresholdsThe COM stone ablation threshold for the Ho:YAG and TFL measured 82.6 J/cm2 and 20.8 J/cm2, respectively. It should be noted that this ablation threshold for the Ho:YAG laser (82.6 J/cm2) is an order of magnitude higher than the value of 7.36 J/cm2, previously reported for COM stones.10 The difference in reported ablation threshold values may be due in part to several factors. First, the ablation thresholds were measured using different criteria in the two studies: by recording the smallest measurable mass loss over many (6000) pulses in our study compared with visual confirmation of the smallest mass loss observable for a single pulse in the previous study. Second, a free-electron laser (FEL) was used to determine stone ablation thresholds in the previous study, which has a unique temporal pulse structure (macropulse of 3 to 5 μs consisting of picosecond micropulses) that is significantly different than that of the Ho:YAG laser (macropulse of 350 μs consisting of microsecond micropulses) used in this study and in the clinic. Third, in the previous study a lens was used to focus the laser beam onto the stone sample, while in this study an optical fiber with diverging output beam was used in a similar method as in the clinic. Fourth, in the previous study COM stones were cut with a diamond saw to produce a flat surface and then irradiated in a dry environment, while in this study COM stones with rough surfaces in their natural hydrated state were irradiated, again similar to the method used in the clinic. The difference between the ablation thresholds of the Ho:YAG (82.6 J/cm2) and TFL (20.8 J/cm2) may be due in part to the difference in water absorption coefficients at the two wavelengths8 (μa = 28 versus 160 cm−1) for the bound water component of the stone as well as the surrounding hydrated environment in the urinary tract. Otherwise, the absorption curve for dehydrated human COM stones in the near-infrared from 1500 to 2000 nm is relatively flat and independent of wavelength,11 so the hard tissue component of the stone probably does not directly contribute to the large difference in absorption coefficients for COM stones at the two wavelengths. 4.2.Ablation RatesThe Ho:YAG ablation rate linearly increased with pulse energy, resulting in a COM stone vaporization rate of 100 μg/s at a pulse energy of about 165 mJ. Although these laser pulse energies are still significantly lower than the minimum pulse energies typically used in the clinic (400 to 600 mJ/pulse), it should be noted that the Ho:YAG laser pulse energy cannot be indefinitely increased because stone retropulsion, which will be discussed in Sec. 4.3, becomes a problem at higher pulse energies. It should also be mentioned that although commercial Ho:YAG lasers are available with pulse rates up to 50 Hz (e.g., for treatment of BPH), these systems are quite large and expensive and actually consist of multiple Ho:YAG laser heads packaged into one system. This design is necessary because thermal effects occur in the laser rod of a flashlamp-pumped solid-state Ho:YAG laser system, which typically leads to a significant decrease in pulse energy as the pulse rate is increased beyond 10 Hz.12 Although the TFL ablation rate also continued to increase with increasing pulse rate, the rate of increase was not linear. An increase in pulse rate from 10 to 100 Hz did not result in an anticipated ablation rate increase of 10-fold, but instead only a 5-fold increase, from 28 to 140 μg/s. It is possible that some of the stone ablation efficiency lost during operation at high pulse rates was due to absorption of a higher fraction of laser pulses in the saline bath as the fiber was scanned across the stone surface, although this contribution requires further study. Charring of the stone surface was also observed at TFL pulse rates above 100 Hz, most likely as a result of thermal buildup as the stone was kept fixed during the study. However, in a clinical environment involving stone mobility and regular saline irrigation and cooling of the stone surface, efficient TFL operation at pulse rates higher than 100 Hz may be feasible (if stone retropulsion is not a concern) and warrants further study. Nevertheless, operation of the TFL at higher pulse rates still results in an increase in the ablation rate, and at relatively little expense, since the diode-pumped fiber laser is capable of operating at arbitrary pulse rates from 1 to 1000 Hz. 4.3.Retropulsion StudiesRetropulsion with the Ho:YAG laser linearly increased with increasing pulse energy. Retropulsion with the TFL was minimal at pulse rates less than 150 Hz, and then rapidly increased with higher pulse rates. The amount of stone retropulsion that would be considered acceptable in a clinical study is not easy to quantify. However, for the purposes of this study, minimal retropulsion was defined to be a retropulsion distance of less than 2 mm. This value is based in part on the observation that the fiber tip to stone surface working distance needs to be short, insuring near-contact working conditions, for efficient stone vaporization during Ho:YAG lithotripsy. This criteria would imply that Ho:YAG laser settings of greater than 175 mJ with a 270-μm fiber results in significant retropulsion. As mentioned earlier, this energy level is considerably less than the lowest settings of 400 to 600 mJ typically available with a clinical Ho:YAG laser system. Indeed, this study confirms what urologists already experience in the clinic, a significant retropulsion effect that results in the clinician having to waste time “chasing” stone fragments inside the urological tract. TFL settings of greater than 150 Hz resulted in significant retropulsion as well. In summary, if both the ablation rate and retropulsion experimental data are considered in unison rather than as separate studies, the results would indicate that a Ho:YAG pulse energy of 165 mJ (at 10 Hz) capable of minimizing stone retropulsion results in an ablation rate of 100 μg/s. A TFL pulse rate of 100 Hz (at 35 mJ) capable of minimizing stone retropulsion results in an ablation rate of 140 μg/s. Thus, if the urologist is concerned about minimizing stone retropulsion effects at the expense of lower stone ablation rates, then the TFL may represent a viable alternative to the Ho:YAG laser. Previous studies reporting on the optimal set of Ho:YAG laser parameters for efficient lithotripsy with minimal stone retropulsion have reached similar conclusions that operation of the Ho:YAG laser with lower pulse energies and higher pulse rates than typically used in the clinic would also be beneficial.13, 14 Furthermore, recent Ho:YAG laser lithotripsy retropulsion studies have concluded that the use of lower pulse energies, longer pulse durations, higher pulse rates, and smaller optical fiber diameters is the optimal combination of laser parameters for minimizing stone retropulsion.15, 16, 17, 18, 19, 20 A comprehensive study of all of these parameters was beyond the scope of this paper. However, it should be emphasized that, unlike the flashlamp-pumped Ho:YAG laser, the diode-pumped TFL is an ideal laser for operation within the range of laser parameters listed above, due to the TFL's excellent spatial beam profile that allows use of small-core fiber diameters and its operation at arbitrary pulse durations and pulse rates. As mentioned in previous studies,4, 5, 6, 7 cost may represent the largest hurdle to application of the TFL for lithotripsy. The flashlamp-pumped Ho:YAG laser is significantly less expensive than a diode-pumped TFL. However, the results of this study may provide further motivation for the development of more compact, less expensive, pulsed thulium fiber lasers for lithotripsy. 5.ConclusionsThe COM stone ablation threshold for the Ho:YAG and TFL measured 82.6 J/cm2 and 20.8 J/cm2, respectively. Stone retropulsion with the Ho:YAG laser linearly increased with pulse energy. Retropulsion with the TFL was minimal at pulse rates less than 150 Hz, and then rapidly increased at higher pulse rates. The TFL provided comparable ablation rates to the Ho:YAG laser for pulse energies and pulse rates that lead to minimal retropulsion. With further development, the thulium fiber laser may represent a viable alternative to the conventional holmium:YAG laser for lithotripsy. AcknowledgmentsThis research was supported, in part, by a collaborative research grant between UNC-Charlotte and the Carolinas Medical Center and a faculty research grant from UNC-Charlotte. Richard Blackmon is supported by a National Science Foundation Graduate Fellowship. ReferencesM. S. Pearle, E. A. Calhoun, and
G. C. Curhan,
“Urologic diseases in America project: urolithiasis,”
J. Urol., 173 848
–857
(2005). https://doi.org/10.1097/01.ju.0000152082.14384.d7 Google Scholar
C. S. Saigal, G. Joyce, and
A. R. Timilsina,
“Direct and indirect costs of nephrolithiasis in an employed population: opportunity for disease management,”
Kidney Int., 68 1808
–1814
(2005). https://doi.org/10.1111/j.1523-1755.2005.00599.x Google Scholar
T. H. Brikowski, Y. Lotan, and
M. S. Pearle,
“Climate-related increases in the prevalence of urolithiasis in the United States,”
Proc. Natl. Acad. Sci. U.S.A., 105 9841
–9846
(2008). https://doi.org/10.1073/pnas.0709652105 Google Scholar
N. M. Fried,
“Thulium fiber laser lithotripsy: an in vitro analysis of stone fragmentation using a modulated 110-W thulium fiber laser at 1.94 μm,”
Lasers Surg. Med., 37 53
–58
(2005). https://doi.org/10.1002/lsm.20196 Google Scholar
N. J. Scott, C. M. Cilip, and
N. M. Fried,
“Thulium fiber laser ablation of urinary stones through small-core optical fibers,”
IEEE J. Sel. Top. Quantum Electron., 15 435
–440
(2009). https://doi.org/10.1109/JSTQE.2008.2012133 Google Scholar
R. L. Blackmon, P. B. Irby, and
N. M. Fried,
“Thulium fiber laser lithotripsy using tapered fibers,”
Lasers Surg. Med., 42 45
–50
(2010). https://doi.org/10.1002/lsm.20883 Google Scholar
R. L. Blackmon, P. B. Irby, and
N. M. Fried,
“Holmium:YAG (λ = 2120 nm) versus thulium fiber (λ = 1908 nm) laser lithotripsy,”
Lasers Surg. Med., 42 232
–236
(2010). https://doi.org/10.1002/lsm.20893 Google Scholar
E. D. Jansen, T. G. van Leeuwen, M. Motamedi, C. Borst, and
A. J. Welch,
“Temperature dependence of the absorption coefficient of water for midinfrared laser radiation,”
Lasers Surg. Med., 14 258
–268
(1994). https://doi.org/10.1002/lsm.1900140308 Google Scholar
D. M. Wilson,
“Clinical and laboratory approaches for evaluation of nephrolithiasis,”
J. Urol., 141 770
–774
(1989). Google Scholar
K. F. Chan, D. X. Hammer, B. Choi, J. M. H. Teichman, H. S. McGuff, H. Pratisto, E. D. Jansen, and
A. J. Welch,
“Free electron laser lithotripsy: threshold radiant exposures,”
J. Endourol, 14 161
–167
(2000). https://doi.org/10.1089/end.2000.14.161 Google Scholar
A. Roggan, U. Bindig, W. Wasche, and
F. Zgoda,
“Properties of biological tissues,”
Applied Laser Medicine, 87 Springer-Verlag, Berlin
(2003). Google Scholar
B. Struve and
G. Huber,
“Properties and medical applications of near-IR solid-state lasers,”
J. Physique IV, 1 C7:3–C7:6
(1991). https://doi.org/10.1051/jp4:1991701 Google Scholar
S. S. Spore, J. M. Teichman, N. S. Corbin, P. C. Champion, E. A. Williamson, and
R. D. Glickman,
“Holmium:YAG lithotripsy: optimal power settings,”
J. Endourol, 13
(8), 559
–566
(1999). https://doi.org/10.1089/end.1999.13.559 Google Scholar
L. Jonat, B. Chew, and
J. Teichman,
“Holmium:YAG lithotripsy fragmentation varies with pulse energy,”
J. Endourol., 24 2135
–2136
(2010). Google Scholar
M. D. White, M. E. Moran, C. J. Calvano, A. Borhan-Manesh, and
B. A. Mehlhaff,
“Evaluation of retropulsion caused by holmium:YAG laser with various power settings and fibers,”
J. Endourol, 12 183
–186
(1998). https://doi.org/10.1089/end.1998.12.183 Google Scholar
H. Lee, T. R. Ryan, J. M. H. Teichman, J. Kim, B. Choi, N. V. Arakeri, and
A. J. Welch,
“Stone retropulsion during holmium:YAG lithotripsy,”
J. Urol., 169 881
–885
(2003). https://doi.org/10.1097/01.ju.0000046367.49923.c6 Google Scholar
D. S. Finley, J. Petersen, C. Abdelshehid, M. Ahlering, D. Chou, J. Borin, L. Eichel, E. McDougall, and
R. V. Cayman,
“Effect of holmium:YAG laser pulse width on lithotripsy retropulsion in vitro,”
J. Endourol, 19 1041
–1044
(2005). https://doi.org/10.1089/end.2005.19.1041 Google Scholar
C. G. Marguet, J. C. Sung, W. P. Springhart, J. O. L’Esperance, S. Zhou, P. Zhong, D. M. Albala, and
G. M. Preminger,
“In vitro comparison of stone retropulsion and fragmentation of the frequency doubled, double pulse Nd:YAG laser and the holmium:YAG laser,”
J. Urol., 173 1797
–1800
(2005). https://doi.org/10.1097/01.ju.0000154341.08206.69 Google Scholar
J. W. Kang, H. Lee, J. M. H. Teichman, J. Oh, J. Kim, and
A. J. Welch,
“Dependence of calculus retropulsion on pulse duration during Ho:YAG laser Lithotripsy,”
Lasers Surg. Med., 38 762
–772
(2006). https://doi.org/10.1002/lsm.20376 Google Scholar
P. Karla, N. Le, and
D. Bagley,
“Effect of pulse width on object movement in vitro using Ho:YAG laser,”
J. Endourol, 21 228
–231
(2007). https://doi.org/10.1089/end.2005.1130 Google Scholar
|