
|
|
1.IntroductionSince the first reported use of the laser in intracanal walls by Weichman and Johnson in 1971, the increase of high-temperature values has been noted during irradiation.1 This increase can compromise the surround tissues, causing periodontal ligament and bone necrosis and tooth ankylosis. However, it is known that laser irradiation has brought important improvements to dentistry and endodontic procedures because of its disinfection capacity and the structural it promotes.2–6 Moritz et al. have stated that laser energy can penetrate into dentinal tubules up to 1000 µm, compared with the 100 µm that an irrigating solution can achieve.7 Therefore, several studies have been conducted to establish safe parameters of laser irradiation in dentistry, not only in the inner surface but also on the outer surfaces of the dental root.8,9 Mostly in endodontics, the use of high-intensity diode lasers has been improving treatment outcomes as an adjuvant in bacteria reduction, removal of smear layer, and sealing improvement.8–10 Also, researchers have reported in the literature that intracanal laser irradiation can increase the temperature up to 7 to 10 °C without causing any damage to periodontal tissues or ligaments.8,9,11 However, the same protocol of irradiation cannot be used for all types of teeth, owing to the extreme difference of thickness between them, especially after endodontic enlargement procedures. Mandibular incisors have thin root walls and become even thinner after endodontic instrumentation. In these cases, some protocols for irradiation that are safe for most teeth could be harmful to the surrounding tissues. The literature on this topic comprises insufficient and poorly described studies of intracanal laser irradiation using mandibular incisors. In this study, we aimed to evaluate the effect of increases in temperature on the outer surfaces of mandibular incisors using different irradiation parameters using intracanal 810-nm high-intensity diode laser irradiation. 2.Materials and MethodsThis study was approved by the local ethics committee at our Institution. Fifty single-rooted fresh mandibular human incisors, recently extracted, were used. They were cleaned with pumice, washed under running water, and kept in distilled water to maintain the level of hydration. After coronal access, a size 15 K-file (Dentsply Maillefer, Baillaigues, Switzerland) was inserted into the root canal down to the apical foramen, and the working length was established 1.0 mm short. All teeth were prepared in a crown-down fashion using K hand files (Dentsply Maillefer) up to a size No. 40 file in association with 2.5% sodium hypochlorite (NaOCl). After that, the root canals were flushed with 10 ml of 2.5% NaOCl, followed by 10 ml of 17% EDTA-T solution (ethylenediaminetetraacetic acid with 0.2% lauryl sodium sulfate biologic detergent), and then rinsed with 20 ml of sterile water to remove the other irrigants. Next, samples were randomly divided into five experimental groups () according to the output power used (1.5, 2.0, 2.5, 3.0, and 3.5 W), in continuous mode. All samples were fixed in a device and immersed in saline solution at 37 °C for 1 h to standardize all root temperatures (Fig. 1). Thermopar K-type sensors (Center Technology Corp., Taipei, Taiwan) were placed on four points of each root (the apical and middle thirds of the mesial and distal sides). The apical third sensors were placed 3 mm from the working length. The middle third sensors were placed over the thinnest root surface (approximately 6 to 7 mm from the working length). Fig. 1Device used to fix the root and keep it immersed in saline solution at 37 °C. Two plastic tubes were placed on each root side to put the thermopar sensors in position. 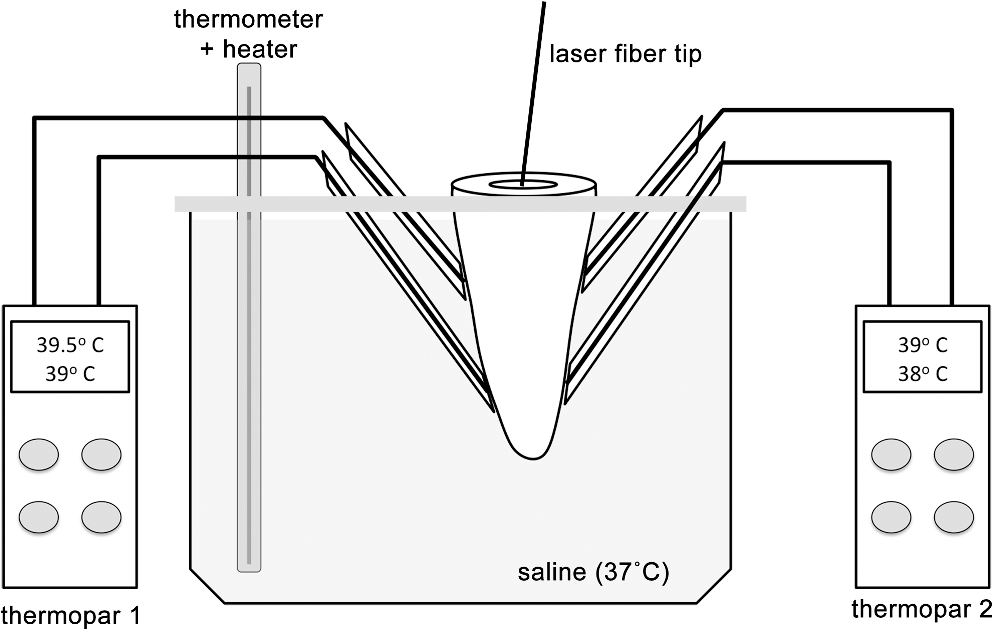 An 810 nm () GaAlAs diode-pumped laser device (Twilight; Biolase Technology, Inc., Irvine, CA, USA) with a 0.40-mm-diameter optical fiber tip was used to irradiate the samples. The root canal was dried before each laser irradiation. The fiber tip was introduced at the working length without activating the laser. The laser equipment was then activated with the fiber tip in contact mode while being moved coronally in circular movements over the root canal wall at (calculated according to the working length of each tooth, based on a time of irradiation).12 This procedure was repeated four times at 20-s intervals. The elevation of the temperature was measured on the apical and middle thirds of the mesial and distal sides. The mean value between the two sides was tabulated. The normality of the data was confirmed by using the Kolmogorov-Smirnov test, then analysis of variance (ANOVA) and Tukey’s test were used to compare differences between the apical and middle thirds for each parameter and between them. 3.ResultsANOVA complemented by Tukey’s test showed no statistical differences between the measured values for all laser settings used in the apical and middle thirds (). In the apical third, the results from the measured values showed that all laser parameters tested differed from each other. The increase in output power resulted in a significant increase of the mean temperature increase. In the middle third, the power levels of 1.5 and 2.0 W presented no statistical differences; however, the other comparisons showed differences (). When we compared the apical and middle thirds of each parameter separately, we found that the increased temperature of middle third was significantly higher than the apical third () in all groups. The only output power that increased the outer surface temperature above 7 °C was 3.5 W in the middle third (Fig. 2). 4.DiscussionReports in the literature have shown the benefits of intracanal high-intensity diode laser irradiation as an adjunct to endodontic therapy.6 Such benefits rely on the antibacterial capacity of this treatment modality and the improvement in the sealing ability of sealants as a result of the structural changes caused on dentin surface.4,7,8,10–14 Although laser irradiation has many advantages, this procedure must be conducted within safe parameters, because an uncontrolled temperature increase could be harmful to surrounding tissues, causing periodontal and bone necrosis at levels higher than 10 °C.8,9,11 In the present study, we considered a temperature variation below 7 °C to be secure. Thermal studies of intracanal laser irradiation normally are conducted in thicker dentin walls, more commonly on upper incisors and premolars.8,9,15 For the present study, we decided to use mandibular incisors because of their thinner dentin walls. Such an anatomic condition is hypothesized to transmit higher temperatures to periodontal tissues. Thus, if an irradiation protocol is secure for this kind of teeth, it can also be used for almost any teeth. The output power used in this experiment was based on the results of previous studies that showed its safe use on thicker teeth surfaces.8 Also, a 20-s interval between irradiation doses was affirmed as essential for significant decreases in temperature, allowing several repetitions for each tooth.11 Da Costa-Ribeiro et al.11 achieved similar results when mandibular incisors were irradiated with 2.5 W. The importance of an interval between irradiations was also proved when we compared the rate of temperature increase of each repetition and did not find significant differences between any of the groups. In all groups, we found that the temperature elevation was significantly higher in the middle third compared to the apical third on the basis of ANOVA. Our results show that just the parameter of 3.5 W in continuous mode protocol increased external surface temperature above 7 °C in the middle third and reached more than 9 °C variation during four irradiations (Fig. 2). These data are in accord with those in other reports in the literature. Hmud et al.16 found that both the diode lasers used in their study (940 and 980 nm) induced only modest temperature changes on the external root surface at the settings used ( and ). Even though the temperature of the water within the canal increased during lasing by as much as 30 °C, the external root surface temperature increased by only a maximum of 4 °C. Irrigation between laser exposures was highly effective in minimizing thermal changes within the root canal and on the root surface. Also, Alfredo et al.17 showed that the irradiation of a 980-nm diode laser in the root at 1.5 and 3.0 W for 20 s can safely be used in endodontic treatment, regardless of the presence of humidity. Taking these findings into account, some parameters used in our study can be considered critical, and they should not be used for clinical procedures. The results obtained with the lower parameters can be safely extrapolated in clinical conditions, however, even in patients with thicker root canal walls. On the basis of the results of this study, we report that the 810-nm high-intensity diode laser can safely be used for endodontic applications with output power up to 3.0 W on thin root canal walls. ReferencesJ. A. WeichmanF. M. Johnson,
“Laser use in endodontics: a preliminary investigation,”
Oral Surg. Oral Med. Oral Pathol., 31
(3), 416
–420
(1971). http://dx.doi.org/10.1016/0030-4220(71)90164-2 OSOMAE 0030-4220 Google Scholar
N. Gutknechtet al.,
“Long-term clinical evaluation of endodontically treated teeth by Nd:YAG lasers,”
J. Clin. Laser Med. Surg., 14
(1), 7
–11
(1996). JCLSEO Google Scholar
Z. Karlovicet al.,
“Erbium:YAG laser versus ultrasonic in preparation of root-end cavities,”
J. Endod., 31
(11), 821
–823
(2005). http://dx.doi.org/10.1097/01.don.0000158234.33581.e9 0099-2399 Google Scholar
C. de Moura-Nettoet al.,
“Morphologic changes and removal of debris on apical dentin surfaces after Nd:YAG laser and diode laser irradiation,”
Photomed. Laser Surg., 26
(3), 263
–266
(2008). http://dx.doi.org/10.1089/pho.2007.2180 PLDHA8 1549-5418 Google Scholar
E. Altundasaret al.,
“Ultramorphological and histochemical changes after Er,Cr:YSGG laser irradiation and two different irrigation regimes,”
J. Endod., 32
(5), 465
–468
(2006). http://dx.doi.org/10.1016/j.joen.2005.08.005 0099-2399 Google Scholar
U. Schoopet al.,
“Innovative wavelengths in endodontic treatment,”
Lasers Surg. Med., 38
(6), 624
–630
(2006). http://dx.doi.org/10.1002/(ISSN)1096-9101 LSMEDI 0196-8092 Google Scholar
A. Moritzet al.,
“Laser in endodontology,”
J. Oral Laser Appl., 2
(1), 87
–95
(2001). 1473-7809 Google Scholar
A. Moritzet al.,
“In vitro irradiation of infected root canals with a diode laser: Results of microbiologic, infrared spectrometric, and stain penetration examinations,”
Quintessence Int., 28
(3), 205
–209
(1997). DEDIAY 0011-8567 Google Scholar
L. O. RamskoldC. D. FongT. Stromberg,
“Thermal effects and antibacterial properties of energy levels required to sterilize stained root canals with an Nd:YAG laser,”
J. Endod., 23
(2), 96
–100
(1997). http://dx.doi.org/10.1016/S0099-2399(97)80253-1 0099-2399 Google Scholar
A. Moritzet al.,
“Irradiation of infected root canals with a diode laser in vivo: Results of microbiological examinations,”
Laser Surg. Med., 21
(3), 221
–226
(1997). LSMEDI 0196-8092 Google Scholar
A. da Costa Ribeiroet al.,
“Effects of diode laser (810 nm) irradiation on root canal walls: thermographic and morphological studies,”
J. Endod., 33
(3), 252
–255
(2007). 0099-2399 Google Scholar
N. Gutknechtet al.,
“Bactericidal effect of the Nd:YAG laser in in vitro root canals,”
J. Clin. Laser Med. Surg., 14
(2), 77
–80
(1996). http://dx.doi.org/10.1089/clm.1996.14.77 PLDHA8 1549-5418 Google Scholar
C. de Moura-Nettoet al.,
“Influence of Nd:YAG and diode laser irradiation on apical sealing when associated with AH plus and EndoREZ endodontic cements,”
Photomed. Laser Surg., 25
(5), 413
–417
(2007). http://dx.doi.org/10.1089/pho.2007.2083 PLDHA8 1549-5418 Google Scholar
N. Gutknechtet al.,
“A clinical comparison of the bactericidal effect of the diode laser and 5% sodium hypochlorite in necrotic root canals,”
J. Oral Laser Appl., 3
(2), 151
–157
(2002). 1473-7809 Google Scholar
N. Gutknechtet al.,
“Temperature evolution on human teeth root surface after diode laser assisted endodontic treatment,”
Lasers Med. Sci., 20
(2), 99
–103
(2005). http://dx.doi.org/10.1007/s10103-005-0347-9 1435-604X Google Scholar
R. HmudW. A. KahlerL. J. Walsh,
“Temperature changes accompanying near infrared diode laser endodontic treatment of wet canals,”
J. Endod., 36
(5), 908
–911
(2010). http://dx.doi.org/10.1016/j.joen.2010.01.007 0099-2399 Google Scholar
E. Alfredoet al.,
“Temperature variation at the external root surface during 980-nm diode laser irradiation in the root canal,”
J. Dent., 36
(7), 529
–534
(2008). http://dx.doi.org/10.1016/j.jdent.2008.03.009 JDENAB 0300-5712 Google Scholar
|




