
|
|
1.IntroductionThe laser consists of a mixture of the gases carbon dioxide, helium, and nitrogen with the active medium being carbon dioxide. Its wavelength, which can vary from 9 to 11 μm, is compatible with the absorption peak of carbonated hydroxyapatite, the major component of the dental enamel (85%).1 Hence, this laser is the most suitable to prevent caries:2–6 its light greatly interacts with enamel, modifying both the structural and chemical compositions of this tissue.7,8 However, to date, a clinical protocol to treat patients does not exist; professionals have controversial opinions regarding power density, irradiation distance from the surface, irradiation time,9 and need to repeat laser irradiation on a previously treated surface. Moreover, the same wavelength range interacts with the water present in the tissue, raising the temperature at irradiated sites and surrounding tissues. Therefore, it is necessary to employ parameters that maintain tissue health by keeping the pulp tissue unaltered. Using laser irradiation to promote chemical changes in tooth enamel and thus to prevent caries increases the temperature in the irradiated tissue.10 Enamel absorbs laser beam radiation—according to the Beer–Lambert law—the larger the radiation wavelength absorption coefficient, the greater the potential to heat the tissue11 and the smaller the penetration depth.12 The temperature rise is important to treat the tissue, because it removes carbonate radicals from the mineral structure8 and modifies the crystal structure.10 Unfortunately, temperature elevation at the irradiation site can degrade the surrounding tissue, so selecting efficient and safe parameters is the main concern when employing different laser wavelengths, energy density, energy per pulse, pulse duration, and irradiation time. The mechanical removal of biofilms by brushing has a potential adverse effect: mineralized tooth tissue abrasion.13 Laser interacts with the tissue rather superficially, and thus radiation does not penetrate deep into enamel. This culminates in rather superficial carbonate loss and structural changes in the tissue. In this context, it is relevant to determine how effectively treatment with laser enhances enamel resistance to acid after brushing. Therefore, this study aimed to assess how brushing affects the laser-irradiated enamel microhardness after cariogenic challenge in vitro. 2.Materials and Methods2.1.Experimental DesignWe investigated surface treatment at four levels: Group 1 (G1)—control, Group 2 (G2)— laser, Group 3 (G3)—brushing, and Group 4 (G4)— . The experimental units consisted of 40 enamel blocks obtained from the occlusal and lingual surfaces of nonerupted human third-molar teeth. The sample size was determined by the statistics program SigmaStat 3.5; a desired maximum error of 20% and an acceptable standard deviation of 30% of the average data were considered. This statistical evaluation provided nine samples per group for a confidence level of 95%. Bearing in mind that loss was possible, 10 samples were selected per group. The specimens were randomly assigned to four groups () according to the surface treatment they were submitted to. The response variable was the enamel cross-sectional Knoop microhardness test at 10, 30, 50, 70, 90, and 110 μm from the surface. 2.2.Sample PreparationTwenty nonerupted third molars (from the Human Tooth Bank of the Ribeirão Preto School of Dentistry-USP) stored in distilled water were used in this study. The teeth were thoroughly cleaned with a hand scaler and rubber cup/pumice prophylaxis; they were then maintained in distilled water at 4°C until use. The teeth were sectioned with the aid of a water-cooled diamond saw in a sectioning machine (Minitom, Struers A/S, Copenhagen, Denmark), so that 40 fragments from buccal and lingual surfaces measuring were obtained from the crown. The specimens were embedded in acrylic resin using polyvinyl chloride rings (Fig. 1). The enamel surfaces were manually finished and polished with 1200-grit silicon carbide paper (Hermes Abrasives Ltd., Virginia Beach, Virginia) under water cooling and then with 0.3 and 0.05 μm alumina paste on cloth, which was followed by ultrasonic cleaning. 2.3.Laser IrradiationAfter sample preparation, the specimens were divided into four groups: G1, G2, G3, and G4. Samples belonging to G2 and G4 were submitted to laser irradiation; G1 and G3 specimens were not irradiated (Fig. 1). Irradiation was conducted with a laser system emitting at a wavelength of 10.6 μm (PC015D, Shangai Jue Hua Laser Technology Development Co., Shangai, China). The laser beam was delivered in the noncontact mode. The irradiation distance from the target site was 4 mm. The parameter settings were as follows: , energy per , , and . The emitted power was measured as 0.55 W by means of a power meter (Coherent Field Max II; Coherent, Santa Clara, California). Using the knife-edge method and considering the Gaussian distribution and the laser beam radial symmetry, the beam diameter at of the intensity level was determined as being 0.31 cm; so, the mean irradiance and the energy density could be appropriately determined as and , respectively. 2.4.Brushing—Abrasive WearSamples belonging to G3 and G4 were submitted to the brushing simulation (Fig. 1), which was performed with a brushing machine (MSET-Marcelo Nucci ME, São Carlos, SP, Brazil) that simulates the horizontal brushing technique. Soft bristle brushes were used (Colgate Classic, Colgate-Palmolive Co., São Bernardo do Campo, SP, Brazil); the specimens were positioned perpendicular to the brushes and were brushed for 80,000 strokes in a reciprocal-action brushing simulator. The load employed on the sample during the cycling process was approximately 300 g. A solution (slurry) obtained by mixing a silica-based dentifrice with low abrasivity [relative enamel ] (Colgate Total 12, Colgate-Palmolive Co., São Bernardo do Campo, SP, Brazil) and distilled water at a 1:3 weight ratio, respectively, were used in the brushing process; this slurry was prepared 20 min before the beginning of the cycling process. The simulation speed was 4.5 strokes per second, and the amplitude excursion was 25 mm. Experiments were run at 37°C ().14 2.5.Acid ChallengeAfter the brushing simulation, all the specimens were subjected to an in vitro model that induces caries-like lesions by pH cycling (Fig. 1). The pH cycling was conducted according to the model proposed by Vieira et al.15 The individual samples were immersed in demineralizing solution ( acetate buffer containing Ca, P, and , pH 5.0) for 6 h, were removed thereafter, washed with distilled and deionized water for 10 s, and lightly dried with a paper towel. Then, the samples were immersed in remineralizing solution ( Ca, P, KCl, in Tris buffer, pH 7.0.) for 18 h. The proportion of demineralizing and remineralizing solutions per area of block was 6.25 and , respectively. The whole procedure was performed at 37°C. The pH-cycling regimen lasted 8 days; on day 4, the de- and remineralizing solutions were replaced with fresh ones. After the eighth-day cycle, the blocks remained in the remineralizing solution for additional 24 h until analyses. 2.6.Microhardness KnoopAfter the in vitro acid challenge, the specimens were ultrasonically cleaned (3L; Dabi Atlante, Ribeirão Preto, SP, Brazil) for 15 min and sectioned in the cervical-occlusal direction in their central portion (Fig. 1). Sectioning was carried out using a diamond disc mounted in the sectioning machine (Minitrom, Struers A/S, Copenhagen, Denmark); one of the sections was embedded in polyester resin to expose the sectioned surface for polishing. The samples were finished and polished with 600 and 1200-grit silicon carbide papers in a polishing machine (DP-9U2, Panambra/Strues, A/S, Copenhagem, Denmark) under water cooling, and then with 0.3 and 0.05 μm alumina pastes applied on a cloth. Next, the resin cylinders containing the specimens were ultrasonically cleaned. The demineralization was quantitatively evaluated by cross-sectional microhardness tests (HMV-2000; Shimadzu Corporation, Kyoto, Japan) (Fig. 1), and the samples were indented using a Knoop diamond under a 25 g load for 10 s to maintain the tip of the indenter parallel to the enamel subsurface. The measurements were accomplished at different subsurface depths—10, 30, 50, 70, 90, and 110 μm from the outer enamel surface. Three indentations equally spaced to the adjacent indentations were taken, and the average was calculated. 2.7.Statistical AnalysisFor statistical analysis of the microhardness data, the area under the curve () was calculated by numerical integration over 10 and 110 μm range using the trapezoidal rule, which was performed using the OriginPro 8.0 program. First, each group was evaluated to identify a normal and homogeneous distribution. Comparison between groups was made using one-way ANOVA. Fisher’s least significant difference (LSD) test was employed to compare the mean values at a significance level of 5%. 3.ResultsConcerning the areas under the microhardness curves (), groups G1 (), G3 (), and G4 () were statistically similar and presented higher demineralization rates. Group G2 () furnished the highest numerical data and hence the lowest demineralization rate (Fig. 2). Fig. 2Microhardness evaluated according the distance from the enamel outer surface and the respective standard deviations. 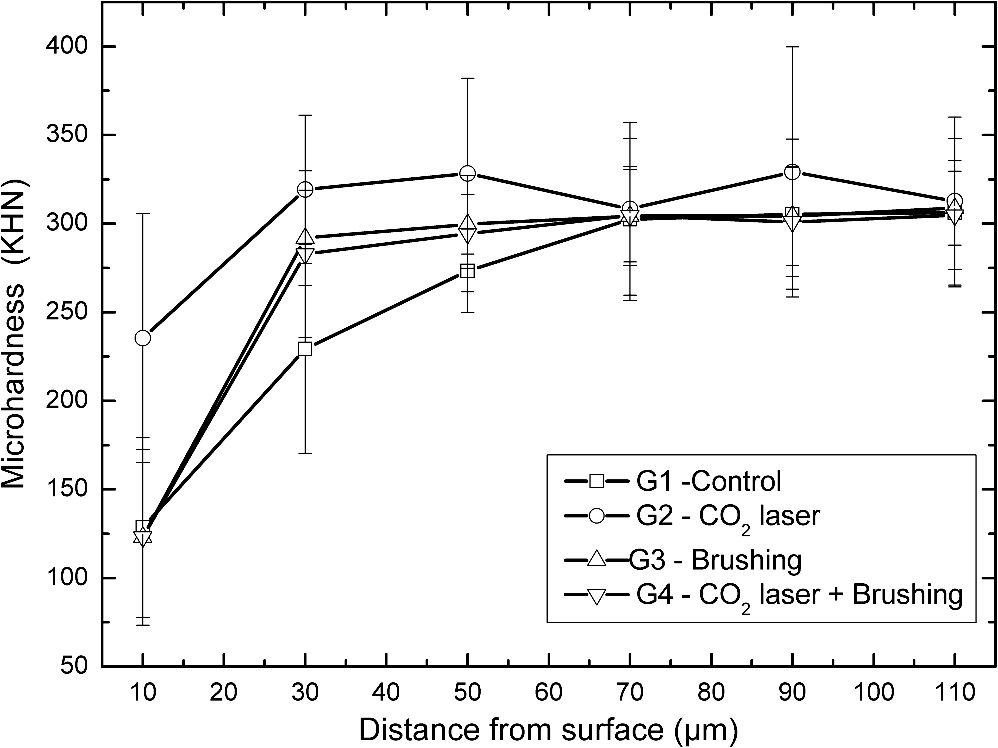 Regarding each specific distance from the surface, at 10 μm the G2 specimens, treated with laser, behaved differently from the other specimens, which were similar. At 30 μm, groups G2, G3, and G4 were similar, but G2 and G3 differed from the control group G1. At 50 μm, only G1 differed from G2. At other distances, the groups were similar (Table 1). Table 1Mean and standard deviation of microhardness data for each distance from the enamel surface (KHN).
Same letters denote statistical similarity—comparison in the rows. 4.DiscussionMany studies have investigated how the laser acts in preventive dentistry. Researchers have noted promising caries-prevention results when irradiating the enamel surface with different wavelengths of this laser. Preventive treatment with laser potentially increases the tooth enamel resistance to acid by avoiding the tissue dissolution caused by acids originated from bacterial metabolism in the biofilm present on the tooth surface.5,8,16,17 Previous studies8,9 have reported altered enamel spectroscopic features, revealing decreased carbonate content following laser irradiation. This chemical modification seems to be one of the effects underlying increased tooth enamel resistance to acid. Here, we verified higher resistance to acid when we treated the enamel with laser. After treatment, we simulated about a 2-year tooth brushing period using a silica-based dentifrice with low abrasivity. The laser-treated specimens submitted to brushing cycles presented demineralization similar to that found for the untreated groups when they were subjected to a pH-cycling model to produce caries-like lesions. Detailed analysis considering the distance of the tested site from the enamel surface showed that the investigated groups presented significantly different microhardness values at 10 μm from the enamel surface, where the carious lesion was more evident. At 30 μm, both groups submitted to brushing (G3 and G4) were statistically similar to G2 specimens irradiated with laser. This result is probably due to the presence of fluoride in the slurry employed during brushing simulation, showing how fluoride affects brushing. We used a dentifrice containing fluoride because we wished to reproduce the reality during the brushing simulation, since treated patients generally use this type of dentifrice. Despite the fluoride effect, we did not observe any enhancement in laser treatment elicited by this element. An analysis employing a lower number of brushing strokes might detect an association between the laser and the fluoride effects on carbonate loss. We shall design future investigations involving the same groups as well as groups submitted to different cycling regimes to establish the number of strokes that are necessary to remove the protective enamel layer generated by laser. Regarding abrasive wear, some studies have demonstrated that the abrasion caused by the bristles of a toothbrush as well as the contact with the dentifrice wears off the enamel.18–21 Although this wear does not represent significant enamel loss, it can reach between 0.05 and 0.20 μm after 1 month of brushing, depending on the dental cream abrasiveness.18–20 Franzó et al. numerically determined this wear: it ranged from 0.03 to 0.11 μm for 3000 cycles of enamel brushing.21 The enamel wear observed in previous studies18–21 showed that brushing had little abrasive effect on the tooth enamel, at least with respect to oral health. However, laser irradiation benefited the patient because it altered the chemical composition and the structure of the enamel tissue. Hence, though small, the wear may be critical, which may incur laser treatment loss. The effectiveness and safety of the laser treatment depend on its therapeutic effect reaching only a thin layer of the enamel surface; the professional must ensure that the temperature rise does not reach the pulp. The laser with a wavelength of 10.6 μm has high-absorption coefficient——because it strongly interacts with the phosphate radical and water.22 This absorption coefficient allows laser radiation to penetrate only a little, 12 μm, for the employed wavelength.23,24 Laser irradiation concentration in a thin 12-μm layer markedly increases the temperature on the enamel surface, producing a higher effect at this site; it also protects the tooth pulp from an undesirable temperature rise, preserving its vitality. The substrate, energy density, pulse width, and total deposited energy greatly influence absolute temperature values on the irradiated surface. Considering literature results employing the laser 10.6 μm using subablative parameters, we can draw some conclusions. In a study about 10.6 μm -laser irradiation, Zuerlein et al.24 observed temperature peaks of 1200°C on the enamel surface irradiated site, 1000°C at 5 μm below the surface, and 400°C at 20 μm below the surface when they used 2 μs and . Carbonate loss possibly occurs at temperatures of about 400°C, but it is more evident at temperatures exceeding 800°C. In addition to the chemical alteration, it is possible to verify structural changes that also take place at temperatures above 600°C.25,26 Zurlein et al. also observed reduced carbonate amount at depths between 4 and 6 μm when they used the aforementioned parameters. Therefore, we can infer that the carbonate loss and a possible irradiated enamel structural alteration are restricted to enamel layers below 6 μm, probably close to the results of Zuerlein et al.,24,27 or even to a thinner layer. Considering the results from previous studies and the findings of the present investigation, we can conclude that the preventive -laser treatment on the tooth enamel is extremely superficial. Hence, professionals should consider enamel wear caused by daily tooth brushing when establishing a clinical protocol to reapply laser after a certain period. More studies are necessary to clarify the ideal time to conduct laser irradiation re-treatment. AcknowledgmentsThis work was partly supported by Grants #2003/13489-6, #2010/06861-0, and #2012/02460-6, São Paulo Research Foundation (FAPESP). The authors thank Dra. Daniela Rios from the Bauru School of Dentistry, University of São Paulo for her cooperation during the brushing process and Cynthia Maria de Campos Prado Manso for linguistic advice. ReferencesR. Z. Legeros,
“Chemical and crystallographic events in the caries process,”
J. Dent. Res., 69 567
–574
(1990). JDREAF 0022-0345 Google Scholar
J. D. B. Featherstoneet al.,
“ laser inhibitor of artificial caries-like lesion progression in dental enamel,”
J. Dent. Res., 77
(6), 1397
–1403
(1998). http://dx.doi.org/10.1177/00220345980770060401 JDREAF 0022-0345 Google Scholar
Z. KantorowitzJ. D. B. FeatherstoneD. Fried,
“Caries prevention by laser treatment: dependency on the number of pulses used,”
J. Am. Dent. Assoc., 129
(5), 585
–591
(1998). Google Scholar
C. Y. Hsuet al.,
“Effects of low-energy laser irradiation and the organic matrix on inhibition of enamel demineralization,”
J. Dent. Res., 79
(9), 1725
–1730
(2000). http://dx.doi.org/10.1177/00220345000790091401 JDREAF 0022-0345 Google Scholar
L. K. Rodrigueset al.,
“Carbon dioxide laser in dental caries prevention,”
J. Dent., 32
(7), 531
–540
(2004). http://dx.doi.org/10.1016/j.jdent.2004.04.004 JDENAB 0300-5712 Google Scholar
C. M. de Souza-e-Silvaet al.,
“Carbon dioxide laser and bonding materials reduce enamel demineralization around orthodontic brackets,”
Lasers Med. Sci., 28
(1), 111
–118
(2013). http://dx.doi.org/10.1007/s10103-012-1076-5 LMSCEZ 1435-604X Google Scholar
C. Steiner-Oliveiraet al.,
“Chemical, morphological and thermal effects of 10.6-microm laser on the inhibition of enamel demineralization,”
Dent. Mater. J., 25
(3), 455
–462
(2006). http://dx.doi.org/10.4012/dmj.25.455 DMJOD5 0287-4547 Google Scholar
A. M. Corrêa-Afonsoet al.,
“FTIR and SEM analysis of laser irradiated human enamel,”
Arch. Oral. Biol., 57
(9), 1153
–1158
(2012). http://dx.doi.org/10.1016/j.archoralbio.2012.02.004 AOBIAR 0003-9969 Google Scholar
M. Esteves-Oliveiraet al.,
“ laser (10.6 micron) parameters for caries prevention in dental enamel,”
Caries Res., 43
(4), 261
–268
(2009). http://dx.doi.org/10.1159/000217858 CAREBK 0008-6568 Google Scholar
B. O. FowlerS. Kuroda,
“Changes in heated and in lased irradiated human tooth enamel and their probable effects on solubility,”
Calcified Tissue Int., 38
(4), 197
–208
(1986). http://dx.doi.org/10.1007/BF02556711 CTINDZ 0171-967X Google Scholar
W. Sekaet al.,
“Light deposition in dental hard tissue and simulated thermal response,”
J. Dent. Res., 74
(4), 1086
–1092
(1995). http://dx.doi.org/10.1177/00220345950740040901 JDREAF 0022-0345 Google Scholar
M. H. Niemz, Laser-Tissue Interactions: Fundamentals and Applications, Springer, Berlin
(1996). Google Scholar
M. AddyM. L. Hunter,
“Can tooth brushing damage your health? Effects on oral and dental tissue?,”
Int. Dent. J., 53
(S3), 177
–186
(2003). http://dx.doi.org/10.1111/idj.2003.53.issue-S3 IDJOAS 0020-6539 Google Scholar
C. P. Turssiet al.,
“Study on the potential inhibition of root dentine wear adjacent to fluoride-containing restorations,”
J. Mater. Sci. Mater. Med., 19
(1), 47
–51
(2008). http://dx.doi.org/10.1007/s10856-007-3140-4 JSMMEL 0957-4530 Google Scholar
A. Vieiraet al.,
“Fluoride dose response in pH-cycling models using bovine enamel,”
Caries Res., 39
(6), 514
–520
(2005). http://dx.doi.org/10.1159/000088189 CAREBK 0008-6568 Google Scholar
A. E. Souza-Gabrielet al.,
“Microhardness and SEM after laser irradiation or fluoride treatment in human and bovine enamel,”
Microsc. Res. Tech., 73
(11), 1030
–1035
(2010). http://dx.doi.org/10.1002/jemt.v73:11 MRTEEO 1059-910X Google Scholar
P. Rechmannet al.,
“Caries inhibition in vital teeth using 9.6-μm -laser irradiation,”
J. Biomed. Opt., 16
(7), 071405
(2011). http://dx.doi.org/10.1117/1.3564908 JBOPFO 1083-3668 Google Scholar
C. J. PhilpottsE. WeaderA. Joiner,
“The measurement in vitro of enamel and dentine wear by toothpastes of different abrasivity,”
Int. Dent. J., 55
(3 Suppl. 1), 183
–187
(2005). IDJOAS 0020-6539 Google Scholar
A. Joineret al.,
“The measurement of enamel and dentine abrasion by tooth whitening products using an in situ model,”
Int. Dent. J., 55
(3 Suppl. 1), 194
–196
(2005). IDJOAS 0020-6539 Google Scholar
A. Joineret al.,
“The measurement of enamel wear by four toothpastes,”
Int. Dent.J., 58
(1), 23
–28
(2008). IDJOAS 0020-6539 Google Scholar
D. Franzòet al.,
“The effect of toothpaste concentration on enamel and dentine wear in vitro,”
J. Dent., 38
(12), 974
–979
(2010). http://dx.doi.org/10.1016/j.jdent.2010.08.010 JDENAB 0300-5712 Google Scholar
D. Friedet al.,
“Thermal and chemical modification of dentin by 9-11-microm laser pulses of 5-100-micros duration,”
Lasers Surg. Med., 31
(4), 275
–282
(2002). http://dx.doi.org/10.1002/(ISSN)1096-9101 LSMEDI 0196-8092 Google Scholar
D. Friedet al.,
“Permanent and transient changes in the reflectance of laser-irradiated dental hard tissues at , 9.6, 10.3, and 10.6 μm and at fluences of ,”
Lasers Surg. Med., 20
(1), 22
–31
(1997). http://dx.doi.org/10.1002/(ISSN)1096-9101 LSMEDI 0196-8092 Google Scholar
M. J. ZuerleinD. FriedJ. D. B. Featherstone,
“Depth profile analysis of the chemical and morphological changes of laser irradiated dental enamel,”
Proc. SPIE, 3593 204
–210
(1999). http://dx.doi.org/10.1117/12.348350 PSISDG 0277-786X Google Scholar
R. Z. LegerosG. BonelR. Legros,
“Types of in human enamel and precipitated apatites,”
Calcified Tissue Res., 26
(2), 111
–118
(1978). http://dx.doi.org/10.1007/BF02013245 CATRBZ 0008-0594 Google Scholar
T. Sakae,
“X-ray diffraction and thermal suties of crystals from the outer and inner layers of human dental enamel,”
Arch. Oral Biol., 33
(10), 707
–713
(1988). http://dx.doi.org/10.1016/0003-9969(88)90003-9 AOBIAR 0003-9969 Google Scholar
M. J. ZuerleinD. FriedJ. D. Featherstone,
“Modeling the modification depth of carbon dioxide laser-treated dental enamel,”
Lasers Surg. Med., 25
(4), 335
–347
(1999). http://dx.doi.org/10.1002/(ISSN)1096-9101 LSMEDI 0196-8092 Google Scholar
|




